Allow assessment of extraintestinal disease
Distend bowel with water ± neutral contrast agent (e.g., VoLumen)
Bolus IV contrast medium at 3-4 mL/sec
•
Noncicatrizing, acute phase
Target or double halo sign
Hyperenhancing inner ring (mucosa)
Low-density middle ring (submucosal edema)
Engorged vasa recta: Comb sign
Proliferation of mesenteric fat and lymphadenopathy
•
Chronic or cicatrizing phase
Strictures, ± dilated small bowel (SB) upstream
Abscesses, fistulas, sinus tracts
•
Barium enema, enteroclysis can depict strictures & fistulas
•
Colonoscopy is best to assess colonic involvement, guide biopsy of colon and terminal ileum
•
Capsule endoscopy may complement imaging studies
Not of proven value following negative CT or MR enterography
Contraindicated in patients with enteric strictures
•
Ulcerative colitis (“backwash” ileitis)
•
Mesenteric enteritis and adenitis
•
Infectious ileitis or colitis
•
Transmural inflammation, lymphoid aggregates, noncaseating granulomas
Predisposes to strictures, fistulas, sinus tracts, abscesses
•
Crohn disease is characterized by intermittent periods of exacerbation of symptoms followed by remissions
•
Complications: Fistulas, sinus tracts, toxic megacolon, obstruction, perforation
•
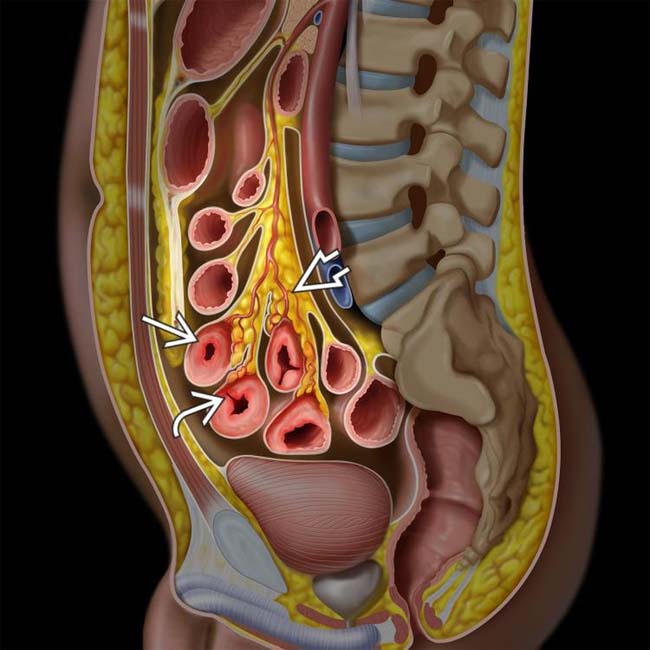
Segmental, discontinuous inflammation of SB ± colon with mucosal hyperenhancement, submucosal edema, engorged vasa recta
•
Consider associated findings (cholangitis, arthritis)
•
Terminal ileitis, regional enteritis, ileocolitis
•
Disease of unknown etiology characterized by transmural inflammation of GI tract
•
Best diagnostic clue
Segmental, discontinuous inflammation of small bowel (SB) ± colon with mucosal hyperenhancement, submucosal edema, engorged vasa recta
–
Usually accompanied by clusters of prominent mesenteric nodes
•
Location
Anywhere along GI tract, from mouth to anus
–
Most common: Terminal ileum (TI) and proximal colon
Distribution
–
80% of patients have SB involvement
–
20% have disease limited to colon
Only 10% have rectal involvement
•
Morphology
Transmural inflammation
–
Predisposes to strictures, fistulas, sinus tracts, abscesses
Skip lesions (segmental or discontinuous)
•
Barium studies: Early changes
“Target” or bull’s-eye appearance of aphthoid ulcerations: Punctate shallow central barium collections surrounded by halo of edema
“Cobblestoning”: Combination of longitudinal and transverse ulcers
Deep fissuring ulcers
Mural thickening: Transmural inflammation, fibrosis
•
Barium studies: Late changes
Skip lesions: Segmental disease with normal intervening segments
Sacculations seen on antimesenteric border
Postinflammatory pseudopolyps, haustral loss, intramural abscess
String sign: Luminal narrowing and ileal stricture
Sinus tracts, fissures, fistulas are hallmarks of disease
Anorectal lesions: Ulcers, fissures, abscesses, hemorrhoids, stenosis
•
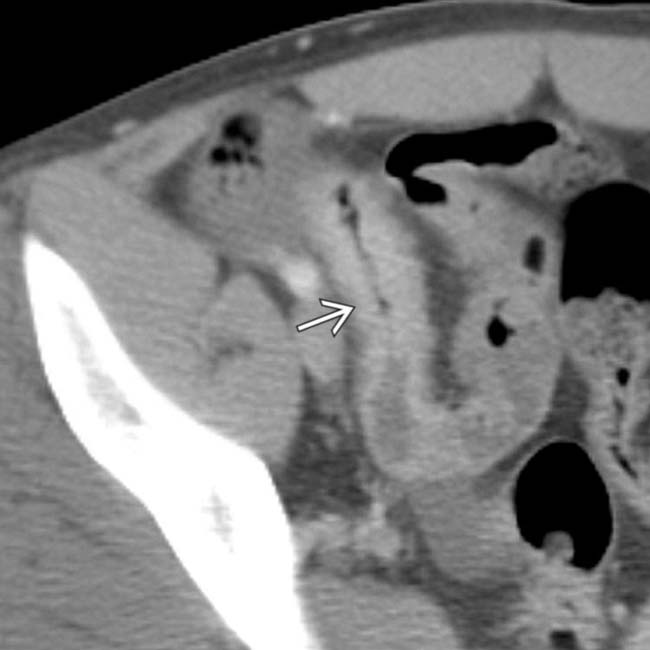
Noncicatrizing, acute phase
Stratified wall thickening of discontinuous SB segments
–
Target or double halo sign
–
Hyperenhancing inner ring (mucosa)
–
Low-density middle ring (submucosal edema)
–
Soft tissue density outer ring (muscularis propria and serosa)
Comb sign: Engorged vasa recta
–
Supply actively inflamed SB segments
Proliferation of mesenteric fat and lymphadenopathy
–
Nodes rarely more than 1 cm in diameter
•
Chronic or cicatrizing phase
Luminal narrowing, ± dilated SB upstream
Mural stratification lost: Indistinct mucosa, submucosa, muscularis propria
–
Alternatively, submucosal fat may proliferate, preserve stratification
Abscesses, fistulas, sinus tracts
–
Fistulas connect 2 epithelialized surfaces (e.g., bowel-to-bowel, bladder, vagina, or skin)
–
Sinus tracts are blind-ending (e.g., bowel to abscess)
Mesenteric changes: Abscess, fibrofatty proliferation, mildly enlarged nodes
Perianal disease: Fistulas and sinus tracts
•
Breath-holding, fat suppression, and gadolinium enhancement show extent and severity of inflammation
Mucosal hyperenhancement, submucosal edema, engorged vasa recta in acute inflammation
•
Allows real-time imaging to assess peristalsis in segments of suspected disease
•
Sensitive in detecting and characterizing
fistulas, sinuses, abscesses in perianal Crohn disease •
Diffusion-weighted imaging can reveal active inflammation even without IV contrast administration
•
Grayscale ultrasound
Transrectal sonography
–
Mural thickening, abscesses, fistulas
–
Anal sphincter heterogeneity
•
Colonoscopy is best modality to assess colon
Often allows inspection and biopsy of terminal ileum













 , transmural inflammation with deep ulcers
, transmural inflammation with deep ulcers  , mesenteric vessel engorgement, and fibrofatty proliferation
, mesenteric vessel engorgement, and fibrofatty proliferation  .
.
 .
.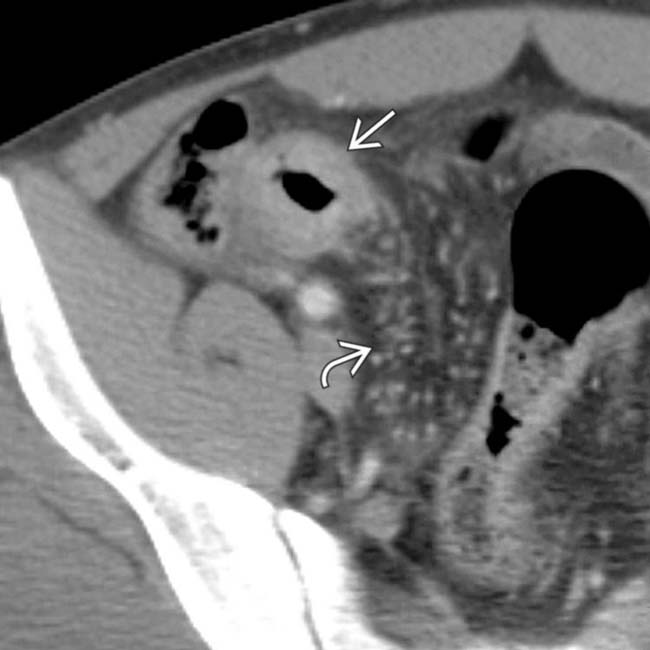
 , as well as local mesenteric fibrofatty proliferation and engorged vasa recta
, as well as local mesenteric fibrofatty proliferation and engorged vasa recta  .
.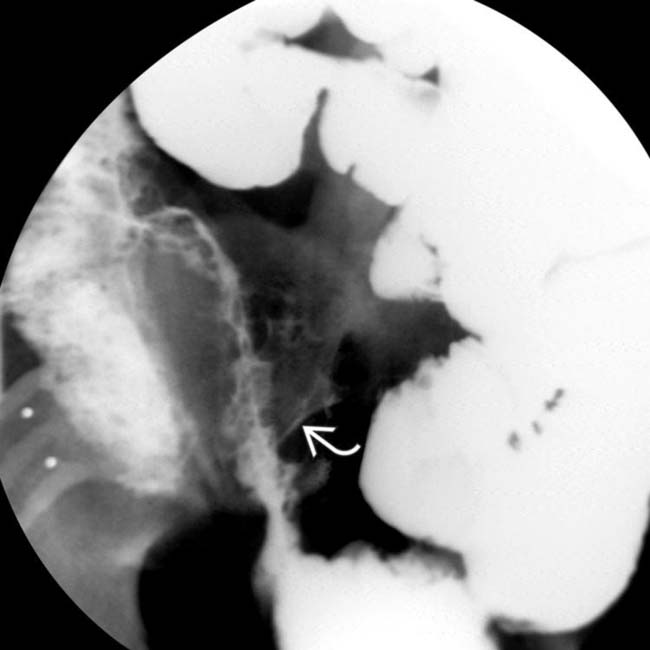
 are opacified. Traditional barium studies remain valuable for evaluation of strictures, fistulas, and sinus tracts.
are opacified. Traditional barium studies remain valuable for evaluation of strictures, fistulas, and sinus tracts.

































