• Divided into syndromic (produce clinical syndrome with abnormal lab findings) or nonsyndromic tumors
• Most common syndromic tumors include insulinoma, glucagonoma, gastrinoma, somatostatinoma, VIPoma
Insulinoma: Usually solitary and benign (90%)
– Presents with Whipple triad (hypoglycemia, low fasting glucose, and relief by IV glucose)
Gastrinoma: Often multiple, malignant (60%), and associated with MEN1
– Presents with Zollinger-Ellison syndrome: Severe peptic ulcer disease, increased acidity, and diarrhea
• Nonsyndromic tumors tend to be malignant (80-100%)
• Treatment
Somatostatin analogs (such as Octreotide) provide symptom relief for syndromic tumors
Surgical resection (enucleation or pancreatectomy), chemoembolization or resection of liver metastases, chemotherapy, and watchful waiting are possible treatment options
(Left) Axial CECT of an insulinoma in the arterial phase shows a subcentimeter hypervascular mass in the pancreatic tail.
(Right) Gross pathology from the same patient shows the resected specimen confirmed to be a neuroendocrine tumor (NET) , with its typical well-circumscribed, noninfiltrative appearance. NETs are often referred to by their main hormonal output (e.g., insulinoma), but pathologists call them NETs because of the electron microscopic finding of neuron-specific enolase.
(Left) Axial CECT in a patient with a metastatic nonsyndromic NET shows a large hypervascular pancreatic mass and additional hepatic metastases . This constellation of findings is typical of a malignant NET of the pancreas, a glucagonoma in this case. Glucagonomas are more commonly malignant than insulinomas.
(Right) Axial CECT demonstrates a cystic lesion in the pancreatic uncinate process. The subtle nodular hypervascular rim around the lesion strongly suggests that this is a cystic NET.
TERMINOLOGY
Abbreviations
• Pancreatic neuroendocrine tumor (NET)
Synonyms
• Islet cell tumor
Definitions
• Tumors arising from pancreatic endocrine cells (islets of Langerhans)
Associated Syndromes
• Multiple endocrine neoplasia type 1 (MEN1, gastrinomas), von Hippel-Lindau syndrome, neurofibromatosis type I, tuberous sclerosis
IMAGING
General Features
• Best diagnostic clue
Well-circumscribed hypervascular pancreatic mass with hypervascular liver metastases
• Location
85% arise in pancreas, while 15% are ectopic
– Most common ectopic locations: Duodenum, stomach, lymph nodes, and ovary
90% of gastrinomas arise in gastrinoma triangle
– Gastrinoma triangle defined by cystic duct and common bile duct (CBD) superiorly, 2nd and 3rd parts of duodenum inferiorly, and pancreatic neck and body medially
– Most commonly arise in duodenal wall
• Size
Varies from few mm to 10 cm
• Morphology
• General concepts
More rare than tumors of exocrine pancreas
Divided into benign (well-differentiated endocrine tumor) or malignant (well/poorly differentiated neuroendocrine carcinoma) based on WHO classification
No longer divided into functioning or nonfunctioning, as all NET are now considered hormonally active
Now divided into syndromic (produce clinical syndrome with abnormal lab findings) or nonsyndromic
– Syndromic tumors: Secrete multiple pancreatic hormones, but patients have single clinical syndrome
PPoma which secretes pancreatic polypeptide does not produce a clinical syndrome
Larger than syndromic tumors at diagnosis due to lack of symptoms or laboratory abnormalities
Cystic NETs more likely to be non-insulin-producing and nonsyndromic
CT Findings
• Well-circumscribed pancreatic mass with noninfiltrative margins that is usually (but not always) hypervascular and most conspicuous on arterial phase
Lesions usually hyperenhance to lesser degree on venous phase, making smaller lesions difficult to detect
– Rarely can be most conspicuous on venous phase
Syndromic tumors tend to be smaller at presentation (usually < 3 cm with insulinomas < 2 cm)
– May be undetectable on NECT and difficult to perceive on venous phase CECT due to small size
Nonsyndromic tumors much larger at presentation (average > 5 cm)
– Usually hypervascular, but less so than syndromic
– Large tumors are more likely to demonstrate central necrosis, cystic change, and calcification
– Liver metastases are often extensive even in asymptomatic patients
Large tumors (syndromic and nonsyndromic) tend to be highly invasive with more aggressive appearance
– Calcification, necrosis, and cystic change more common
– Lesions with early portal vein invasion → widespread liver metastases
• Lesions often demonstrate calcification (central or diffuse)
• Usually no biliary or pancreatic duct obstruction (unless large) or upstream pancreatic atrophy
Some small tumors may rarely secrete serotonin that can cause fibrosis and obstruction of pancreatic duct
• Invasion (rather than encasement) by tumor of mesenteric veins (portal vein or superior mesenteric vein)
• Cystic NET can mimic other pancreatic cystic lesions
Presence of peripheral enhancement or nodularity on arterial phase should strongly suggest diagnosis
• Metastases demonstrate similar characteristics to primary tumor: Hypervascular lymph node and liver metastases
Most common sites of metastases include liver, local lymph nodes, and bone (sclerotic lesions)
Fluid-fluid levels within neuroendocrine liver metastases described as specific feature
• Zollinger-Ellison syndrome (gastrinoma): Avid enhancement and wall thickening of proximal stomach
MR Findings
• NETs tend to be hypointense (relative to normal pancreas) on T1WI, hyperintense on T2WI, and enhance similarly to CECT on T1WI C+ images
Homogeneous enhancement for small tumors < 2 cm
Heterogeneous enhancement with areas of necrosis for larger lesions
• Liver metastases can often be very hyperintense on T2WI and mimic hemangiomas or cysts
Fluid-fluid levels may be visualized within liver metastases, particularly on T2WI
Liver metastases usually T1WI hypointense but may show hyperintensity due to intratumoral hemorrhage
• DWI: Lesions show variable ADC values, but DWI can help identify tiny lesions that are otherwise occult
Ultrasonographic Findings
• Endoscopic US: Sensitivity and specificity > 90%
Can be helpful to identify small NET that may be missed on CT/MR in patients with high clinical suspicion
Can “tattoo” lesion to guide laparoscopic surgery
No specific imaging features, as lesions tend to be hypoechoic or isoechoic to surrounding pancreas
• Intraoperative US: Can detect small nonpalpable lesions and help guide surgical resection
Angiographic Findings
• Functioning and nonfunctioning tumors
Hypervascular (primary and secondary)
• Hepatic venous sampling after arterial stimulation









 in the pancreatic tail.
in the pancreatic tail.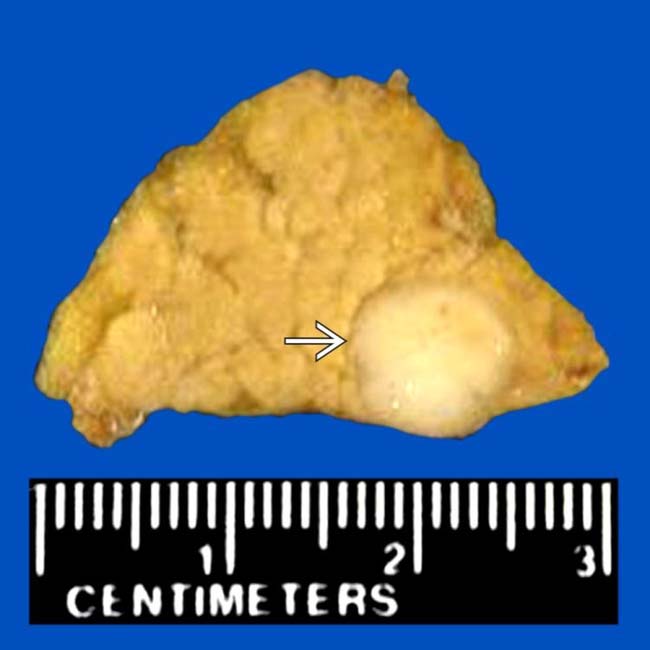
 , with its typical well-circumscribed, noninfiltrative appearance. NETs are often referred to by their main hormonal output (e.g., insulinoma), but pathologists call them NETs because of the electron microscopic finding of neuron-specific enolase.
, with its typical well-circumscribed, noninfiltrative appearance. NETs are often referred to by their main hormonal output (e.g., insulinoma), but pathologists call them NETs because of the electron microscopic finding of neuron-specific enolase.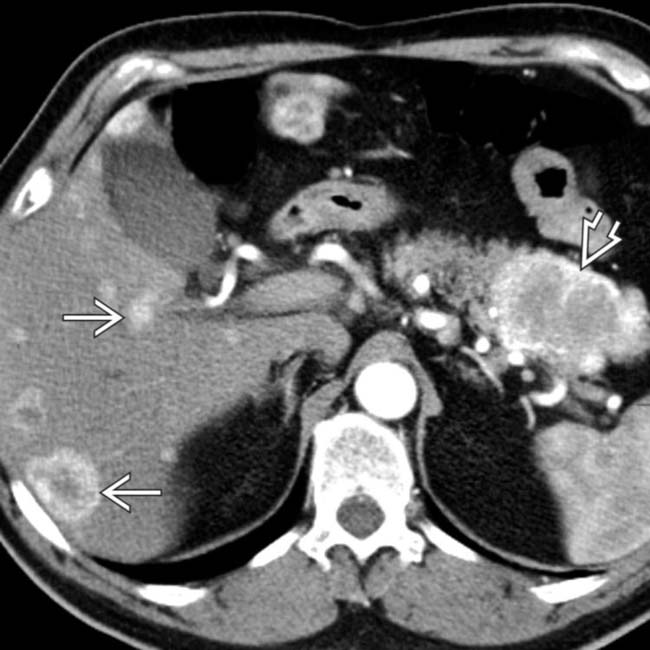
 and additional hepatic metastases
and additional hepatic metastases  . This constellation of findings is typical of a malignant NET of the pancreas, a glucagonoma in this case. Glucagonomas are more commonly malignant than insulinomas.
. This constellation of findings is typical of a malignant NET of the pancreas, a glucagonoma in this case. Glucagonomas are more commonly malignant than insulinomas.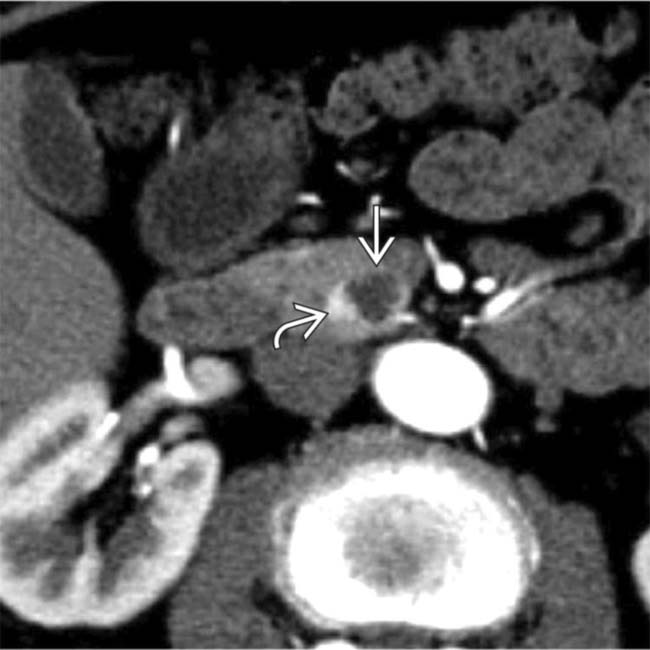
 in the pancreatic uncinate process. The subtle nodular hypervascular rim
in the pancreatic uncinate process. The subtle nodular hypervascular rim  around the lesion strongly suggests that this is a cystic NET.
around the lesion strongly suggests that this is a cystic NET.



 Divided into benign (well-differentiated endocrine tumor) or malignant (well/poorly differentiated neuroendocrine carcinoma) based on WHO classification
Divided into benign (well-differentiated endocrine tumor) or malignant (well/poorly differentiated neuroendocrine carcinoma) based on WHO classification No longer divided into functioning or nonfunctioning, as all NET are now considered hormonally active
No longer divided into functioning or nonfunctioning, as all NET are now considered hormonally active






 Lesions usually hyperenhance to lesser degree on venous phase, making smaller lesions difficult to detect
Lesions usually hyperenhance to lesser degree on venous phase, making smaller lesions difficult to detect 





















