Variable MR signal intensity locules depending on content of cystic fluid
• Malignant potential to develop into cystadenocarcinoma even after years of stability
TOP DIFFERENTIAL DIAGNOSES
• Hemorrhagic or infected hepatic cyst
No enhancement of nodules or septa
• Hepatic pyogenic abscess
Cluster sign: Small abscesses aggregate, sometimes coalesce into single large septate cavity
Rim of abscess locules will enhance
• Cystic metastases
Show debris and mural nodularity
• Hydatid (echinococcal) disease
CLINICAL ISSUES
• Usually occurs in middle-aged women
> 90% in women
DIAGNOSTIC CHECKLIST
• Large, well-defined, homogeneous or heterogeneous, complex cystic mass with septations and nodularity
Almost always solitary
Enhancing mural nodules suggest malignancy
• May mimic hemorrhagic or infected hepatic cyst
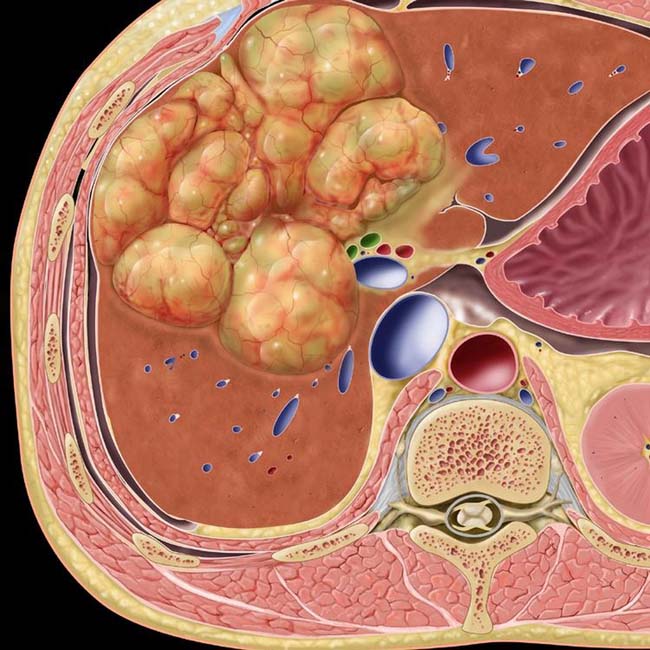
(Left) Graphic shows a lobulated complex cystic mass with a vascularized wall and septa.
(Right) Axial CECT in a middle-aged woman shows a complex cystic mass with lobulated margins and an enhancing wall and septa . These findings in a patient with no other known tumor could be considered sufficiently diagnostic of a biliary cystadenoma to warrant resection without further evaluation.
(Left) Axial T1WI MR in a middle-aged woman shows a classic multiseptate, cystic, hepatic mass with cyst contents having features characteristic of fairly simple fluid. There is slight heterogeneity of the signal that varies between some of the cyst compartments.
(Right) Axial T2WI MR in the same patient shows the bright signal of fluid content within the large septate mass.
TERMINOLOGY
Synonyms
• Bile duct cystadenocarcinoma, hepatobiliary cystadenoma
Definitions
• Rare, malignant or premalignant, unilocular or multilocular, cystic tumor
May arise from intrahepatic bile ducts (IHBDs) within liver (common site)
Very rarely from extrahepatic biliary tree or gallbladder
IMAGING
General Features
• Best diagnostic clue
Complex, multiloculated, cystic mass in liver, often with septations and mural calcifications
• Location
Right lobe (55%), left lobe (29%), both lobes (16%)
Arising from
– Intrahepatic biliary ducts (83%)
– Extrahepatic bile ducts (13%)
– Gallbladder (0.02%)
• Size
1.5-25 cm in diameter
– Usually large at time of diagnosis if symptomatic
• Key concepts
Biliary cystadenocarcinoma
– Malignant transformation of benign biliary cystadenoma
– Typically solitary tumor; usually multilocular, but sometimes unilocular
– Tumor is encapsulated
– Usually seen in middle-aged women
– Recurs after incomplete excision
Benign biliary cystadenoma
– Probably congenital in origin due to presence of aberrant bile ducts
– Recurs after incomplete excision
– Malignant potential to develop into cystadenocarcinoma even after years of stability
Benign and malignant lesions together account for only 5% of all intrahepatic lesions of bile duct origin
Microcystic cystadenoma variant
– Composed of multiple small cysts
– Glycogen-rich cystadenoma
– Typical papillary and mesenchymal stromal features are not seen
– Lined by single layer of cuboidal epithelial cells
– Resembles serous microcystic adenoma of pancreas in pathology and on imaging
CT Findings
• NECT
Large, well-defined, homogeneous, hypodense, water-density mass
– Some are heterogeneous (cystic and hemorrhagic areas)
Cystadenocarcinoma: Septations and nodularity
Cystadenoma: Septations without nodularity
Mural or septal calcifications are common
Biliary dilatation (due to pressure effect) of IHBDs
– Biliary obstruction considered to favor malignant tumor
• CECT
Multilocular tumor
– Nonenhancing cystic spaces
– Enhancement of internal septa, capsule, and nodules
– Enhancement of papillary excrescences
– Mural or septal calcifications
Less commonly, “honeycomb” or “sponge” appearance (microcystic variant)
– Uncommonly has metastases or adenopathy at initial diagnosis
Unilocular tumor
– Large or small nonenhancing cystic space
– Enhancement of outer capsule and papillary excrescences
– Fine mural calcifications
MR Findings
• T1WI
Variable signal intensity locules depending on content of cystic fluid
High signal intensity (mucoid or hemorrhagic fluid)
Low signal intensity (serous fluid)
Septal or mural calcifications: Hypointense
• T2WI
High signal intensity (serous fluid)
Low signal intensity (mucoid fluid)
Only gold members can continue reading. Log In or Register to continue









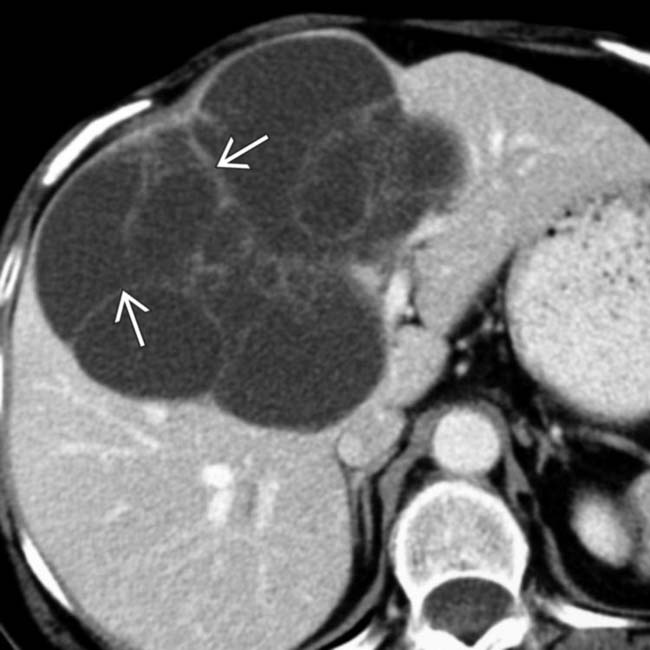
 . These findings in a patient with no other known tumor could be considered sufficiently diagnostic of a biliary cystadenoma to warrant resection without further evaluation.
. These findings in a patient with no other known tumor could be considered sufficiently diagnostic of a biliary cystadenoma to warrant resection without further evaluation.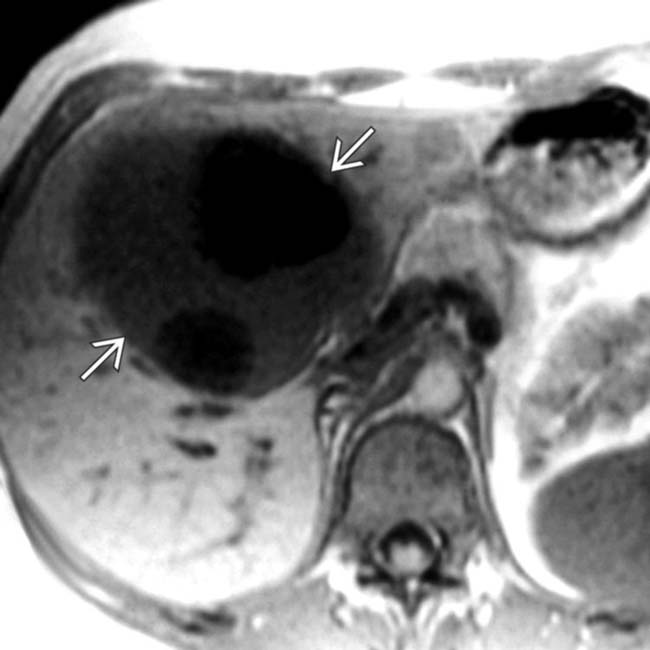
 with cyst contents having features characteristic of fairly simple fluid. There is slight heterogeneity of the signal that varies between some of the cyst compartments.
with cyst contents having features characteristic of fairly simple fluid. There is slight heterogeneity of the signal that varies between some of the cyst compartments.





























