Head and uncinate process of pancreas drained by ventral pancreatic duct of Wirsung via major papilla
Body and tail of pancreas drained by dorsal pancreatic duct of Santorini via minor papilla
• MRCP: Best noninvasive modality for delineating divisum
Dominant dorsal duct, which appears long and narrow, directly entering minor papilla
– Main pancreatic duct may be mildly dilated
Ventral duct appears short and drains into major papilla
No communication between dorsal and ventral ducts
Secretin-enhanced MR/MRCP may help better delineate divisum by distending pancreatic duct
• ERCP: Most accurate method of diagnosing divisum
Cannulation of major papilla reveals opacification of short, tapered, ventral pancreatic (Wirsung) duct
– Contrast does not flow past pancreatic head
Cannulation of minor papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic (Santorini) duct which drains nearly entire pancreas
No communication between dorsal and ventral ducts
• CT: May demonstrate abnormally large pancreatic head or 2 distinct pancreatic moieties separated by fat cleft
CLINICAL ISSUES
• Most common congenital anatomic variant of pancreas
• May be associated with recurrent pancreatitis (mostly in children), although less than 5% are symptomatic
Poor drainage from body and tail (due to relative stenosis at minor papilla) leads to pancreatitis
• Incidental finding in asymptomatic patient: No treatment
• Severely symptomatic patients: Surgical sphincteroplasty or endoscopic papillotomy of minor papilla
(Left) Graphic shows several common variations in the arrangement of the main pancreatic duct , the accessory duct of Santorini , and the duct of Wirsung . The lower right image shows pancreas divisum.
(Right) ERCP image after cannulation of the major papilla demonstrates filling of only a short ventral duct and its side branches. There is no communication with the dorsal duct, compatible with pancreatic divisum.
(Left) ERCP in a patient with pancreas divisum and chronic pancreatitis shows dilatation and irregularity of the dorsal pancreatic duct and small pseudocysts following cannulation of the minor papilla.
(Right) Coronal MRCP shows the dorsal pancreatic duct crossing the common bile duct to drain into the expected location of the minor papilla . The ventral duct is not seen. Note the dilatation of multiple tiny pancreatic duct sidebranches throughout the gland, likely reflecting the patient’s history of chronic pancreatitis.
TERMINOLOGY
Definitions
• Anatomic variant of pancreatic ductal anatomy resulting from failure of ventral and dorsal pancreatic buds to fuse
IMAGING
General Features
• Best diagnostic clue
Normal branching pattern of short ventral duct with no communication between ventral duct and long dorsal duct on ERCP
• Morphology
Most common congenital anatomic variant of pancreas
Most common variant of pancreatic ductal fusion and drainage anomalies
• Normal PD anatomy
Head and uncinate process of pancreas drained by ventral pancreatic duct (PD) of Wirsung via major papilla
Body and tail of pancreas drained by dorsal PD of Santorini via minor papilla
MR Findings
• MRCP is best noninvasive modality for delineating course and drainage pattern of dorsal and ventral PDs
No communication between dorsal and ventral ducts in pancreatic divisum
– Dominant dorsal duct, which appears long and narrow, directly enters minor papilla
Majority of pancreas is thus drained into minor papilla via duct of Santorini
Dorsal duct may have constant, mildly dilated caliber (rather than normal tapering towards tail)
Focal cystic dilatation of duct of Santorini is termed “santorinocele” and easily visible on MRCP
Anatomic relationship between dorsal duct and common bile duct on MRCP MIP reconstruction results in characteristic crossing ducts sign
– Ventral duct appears short and drains into major papilla, with no connection with dorsal duct
Posterior pancreatic head and uncinate drain into major papilla via duct of Wirsung
Main PD may be dilated due to stenosis at minor papilla or repeated bouts of pancreatitis
• Pancreas may demonstrate abnormally high signal on T2WI and low signal on T1WI with peripancreatic free fluid in setting of superimposed pancreatitis
• Secretin-enhanced MRCP may help better delineate divisum by distending PD
Secretin (0.2 μg/kg) induces secretion of bicarbonate-rich fluid from pancreas and increases tone of sphincter of Oddi, thereby distending PD and improving visualization
Secretin-enhanced MR shown to have superior sensitivity/specificity for divisum compared to MR without secretin
CT Findings
• CT had sensitivity/specificity for divisum > 90% in 1 study, but MR is still considered superior
• Delineating pancreatic ductal anatomy is more difficult on CT (compared to MR), but may be aided by multiplanar and minimum intensity projection reconstructions with thin-collimation sections
Dorsal duct, which may be dilated, can be directly traced from pancreatic tail into minor papilla
Ventral duct is smaller (may be difficult to visualize on CT) and drains into major papilla
No communication between ventral and dorsal ducts
• Changes in pancreatic morphology may also suggest divisum, but frequency of findings is low
Abnormal contour of pancreatic head and neck with large pancreatic head
2 distinct pancreatic moieties separated by fat cleft
• Acute or chronic pancreatitis may be present
Enlargement of gland, fat stranding, intra-/peripancreatic cysts, glandular atrophy, parenchymal or ductal calcifications, peripancreatic fat stranding, fluid collections, etc.
Radiographic Findings
• ERCP: Most accurate method of diagnosing divisum, but carries risks of invasive procedure
Cannulation of major papilla reveals opacification of short, tapered, ventral pancreatic duct
– Contrast injected into major papilla does not flow past pancreatic head
– Guidewire inserted into major papilla does not extend past pancreatic head
– Ventral duct maintains normal branching pattern, unlike truncated, abrupt cut-off of ventral duct in pancreatic cancer
Cannulation of minor or accessory papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic duct that drains nearly entire pancreas except posterior head and uncinate
– Cannulation of minor papilla may be technically difficult due to small size
No communication between dorsal (long) and ventral (short) PDs
Ultrasonographic Findings
• Primary limitation is inability to visualize portions of pancreas due to overlying bowel gas
• Secretin test can be performed to identify patients who will benefit from surgical sphincterotomy
Involves sequential US measurements of PD size after secretin administration
– Secretin increases bicarbonate secretion, which overloads functionally inadequate papilla
Only gold members can continue reading. Log In or Register to continue





 Cannulation of major papilla reveals opacification of short, tapered, ventral pancreatic (Wirsung) duct
Cannulation of major papilla reveals opacification of short, tapered, ventral pancreatic (Wirsung) duct Cannulation of minor papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic (Santorini) duct which drains nearly entire pancreas
Cannulation of minor papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic (Santorini) duct which drains nearly entire pancreas

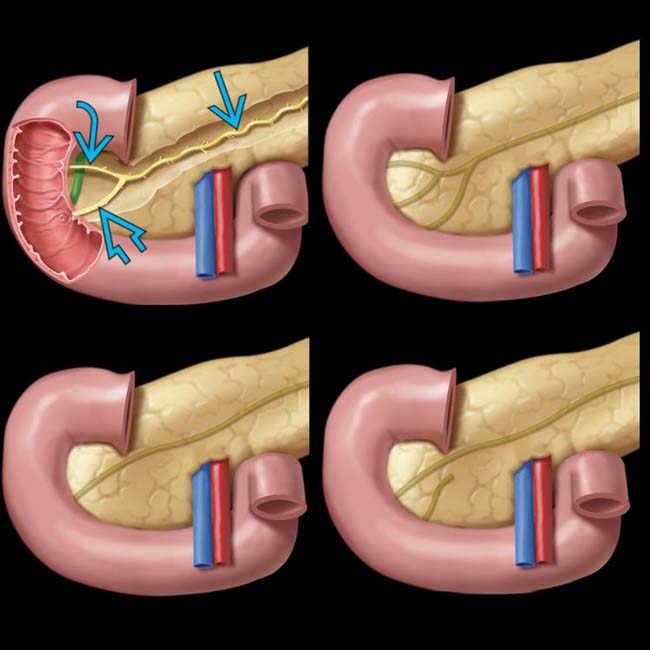
 , the accessory duct of Santorini
, the accessory duct of Santorini  , and the duct of Wirsung
, and the duct of Wirsung  . The lower right image shows pancreas divisum.
. The lower right image shows pancreas divisum.
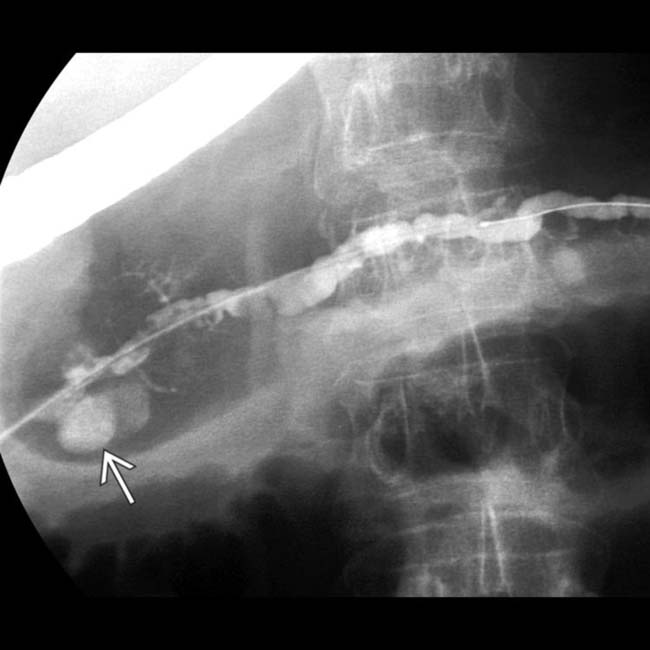
 following cannulation of the minor papilla.
following cannulation of the minor papilla.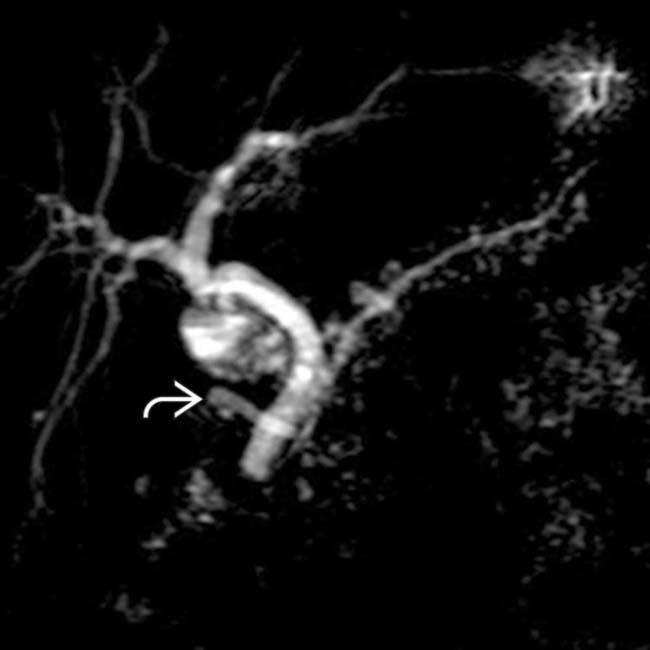
 . The ventral duct is not seen. Note the dilatation of multiple tiny pancreatic duct sidebranches throughout the gland, likely reflecting the patient’s history of chronic pancreatitis.
. The ventral duct is not seen. Note the dilatation of multiple tiny pancreatic duct sidebranches throughout the gland, likely reflecting the patient’s history of chronic pancreatitis.




 No communication between dorsal and ventral ducts in pancreatic divisum
No communication between dorsal and ventral ducts in pancreatic divisum













 Cannulation of minor or accessory papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic duct that drains nearly entire pancreas except posterior head and uncinate
Cannulation of minor or accessory papilla reveals opacification of long (and sometimes dilated) dorsal pancreatic duct that drains nearly entire pancreas except posterior head and uncinate

 Involves sequential US measurements of PD size after secretin administration
Involves sequential US measurements of PD size after secretin administration





