Basic Anatomy
Contrary to likely expectations, this present chapter does not give a comprehensive description of the anatomy of the chest organs. Rather, it highlights a number of anatomic landmarks of interest in routine radiology.
2.1 The Mediastinum
Note 
The mediastinum is the space between left and right lung bordered anteriorly by the sternum, posteriorly by the spinal column, cranially by the superior thoracic aperture, caudally by the diaphragm, and laterally on both sides by the pleura.
The division of the mediastinum into compartments (▶Table 2.1) is of practical importance, in particular, for diagnostic radiology of mediastinal tumors. Differential diagnosis will vary greatly in accordance with tumor localization. The most common systems are the three-compartment model (anterior, middle, and posterior mediastinum) and the four-compartment model (like the three-compartment model, plus superior mediastinum).1 There are other less well-known compartment systems.2
Since there is no rigid border between the described mediastinal compartments, pathologic processes can spread unchecked from one compartment to another.
2.1.1 The Vascular System
Aorta
The thoracic portion of the aorta is divided into three segments:
Ascending aorta: Maximum width of 3.5 cm.
Aortic arch with the origins of the supra-aortic arteries: The most common normal variant—bicarotid trunk (common origin of the brachiocephalic trunk and the left common carotid artery; ▶Fig. 2.1).
Table 2.1 Anatomic compartments of the mediastinum based on the three- and four-compartment model2
Compartments
Border
Three-compartment model
Anterior mediastinum
Space extending from sternum to the anterior surface of the pericardium, ascending aorta, and brachiocephalic vessels
Middle mediastinum
Space between anterior and posterior mediastinum
Posterior mediastinum
Space between the posterior surface of the pericardium and the large vessels extending to the thoracic spine
Four-compartment model
Plus: superior mediastinum
Space above the aortic arch
Descending aorta: Maximum width distal to the aortic arch of 2.6 cm, where it passes the diaphragm maximum 2.4 cm.3
An aortic aneurysm is defined as dilation of the aorta by at least 1.5-fold its normal maximum diameter. The simplified limit values are 5 cm for the ascending aorta and 4.5 cm for the thoracic descending aorta.
Anomalies of the aortic arch are divided into five groups:
Duplicated aortic arch: This can cause compression of the central airways.
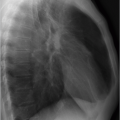
Right-sided aortic arch with mirror-image vascular branching: This should not be misinterpreted on radiographs as a mediastinal mass (▶Fig. 2.2).
Right-sided aortic arch with abnormal vascular branching.
Left aortic arch with abnormal vascular branching: The most common finding here is a lusoria artery, i.e., an aberrant right subclavian artery that branches as the last artery from the aortic arch and runs toward the right in a retroesophageal direction and may lead to impaired swallowing (▶Fig. 2.3).
Cervical aortic arch.
The embryonic ductus Botalli (ductus arteriosus) is a connection between the aortic arch and pulmonary trunk that is obliterated after birth, giving rise to the ligamentum arteriosum, which at times can be identified on computed tomography (CT) as a connective tissue strand (▶Fig. 2.4). In addition to the aortic valve level and the diaphragmatic aortic hiatus, this constitutes the third fixation point for the thoracic aorta. Therefore, this site is particularly susceptible to aortic rupture secondarily to chest injuries (see Chapter 15).
 Fig. 2.1 Bicarotid trunk. CT image. Cranial to the aortic arch, there are only two arterial vessels: the bicarotid trunk (arrow) and the left subclavian artery (arrowhead). |
 Fig. 2.2 Right-sided aortic arch (arrow). Radiograph. |
 Fig. 2.3 Lusoria artery (arrow). CT image. Right subclavian artery running posterior to the esophagus (arrowhead). |

Pulmonary Arteries
Like the aorta, the central pulmonary arteries are elastic-type arteries, while the peripheral pulmonary arteries distal to the segmental arteries are of the muscular type. This is why, following a rise in pressure the central, but not the peripheral, pulmonary arteries appear dilated. On radiographs, amputated hila are seen, in particular, in the presence of underlying chronic obstructive lung disease.
Bronchial Arteries
The lungs have duplicate blood supply: via the large-caliber pulmonary arteries, accounting for the entire cardiac output, and via the small-caliber systemic bronchial arteries supplying the lungs. Their origin is variable but the majority of the left-sided bronchial arteries arise directly from the thoracic aorta, while their right-sided counterparts originate from the third right intercostal artery.4 They course along the bronchi to the periphery.
 Fig. 2.5 Central veins in thorax. Schematic diagram. |
Central Veins
The central thoracic veins are illustrated in ▶Fig. 2.5. The anatomy of the venous system of the chest organs is often brought
to the attention of the radiologist following malpositioning of a central venous catheter.
to the attention of the radiologist following malpositioning of a central venous catheter.
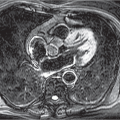
One important anatomic variant is persistent left superior vena cava (▶Fig. 2.6), mainly draining into the coronary sinus. Identification on the radiograph, at the left mediastinal border, of a central venous catheter or pacemaker that had been inserted from the left and now runs caudally is suggestive of such a venous anomaly. Infrequently, it drains into the left atrium or into a pulmonary vein, thus giving rise to a right-left shunt.5
 Fig. 2.6 Persistent left superior vena cava. CT image. Large-caliber venous vessel on the left, lateral to the aortic arch (arrow). |
 Fig. 2.7 Agenesis of the intrahepatic segment of the inferior vena cava. CT image. Extensively dilated azygos vein (arrow) on the right, beside the aorta. |
 Fig. 2.8 Course of the pulmonary veins. CT image. (a) Section somewhat caudal to the tracheal bifurcation: left (arrow) and right superior pulmonary vein (arrowhead). (b) Section at the level of the left atrium: left (arrow) and right inferior pulmonary vein (arrowhead). |
Conspicuous dilation of the azygos vein points to an obstruction or the absence of vasculature in the flow region of the inferior vena cava, often involving agenesis of segments of the inferior vena cava (▶Fig. 2.7).
Pulmonary Veins
Each of the two lungs is drained by two pulmonary veins that terminate in the left atrium. The right lower lobe and middle lobe share a common venous drainage system. ▶Fig. 2.8 shows the course of the central pulmonary veins on CT.
Details of partial anomalous termination of pulmonary veins in systemic veins, resulting in a left-right shunt, are given in Section 19.5.
2.1.2 The Lymphatic System
Conversancy with the lymphatic drainage system of the lungs is paramount in thoracic oncology. Both lungs drain via hilar and mediastinal lymph nodes into the thoracic duct. The latter is generally not identifiable on imaging, apart from the cisterna chyli which can sometimes be seen on CT or MRI between the diaphragmatic crura as a cystic structure measuring several millimeters. The thoracic duct terminates in the left venous angle, i.e., at the confluence of the left internal jugular vein and the subclavian vein.
The IASLC (International Association for the Study of Lung Cancer) nomenclature should be used for naming mediastinal and hilar lymph node stations in the examination reports (▶Table 2.2 and ▶Fig. 2.9).6
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


