Fig. 21.1
Misty mesentery in patient with systemic lupus erythematosus. (a–d) Venous phase axial CT images depict a segmental stranding along the mesentery (arrows) with small lymph nodes (arrowhead)
21.7.2 Mesenteric Panniculitis
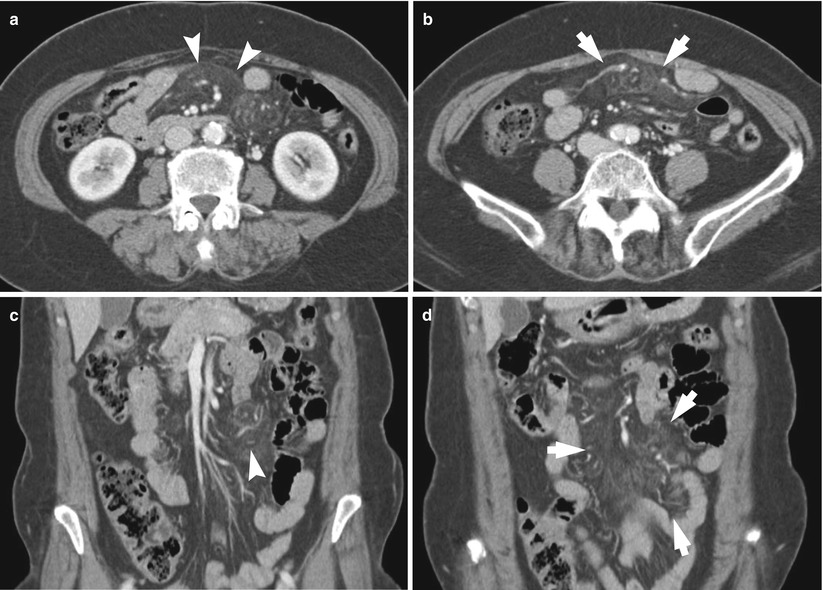
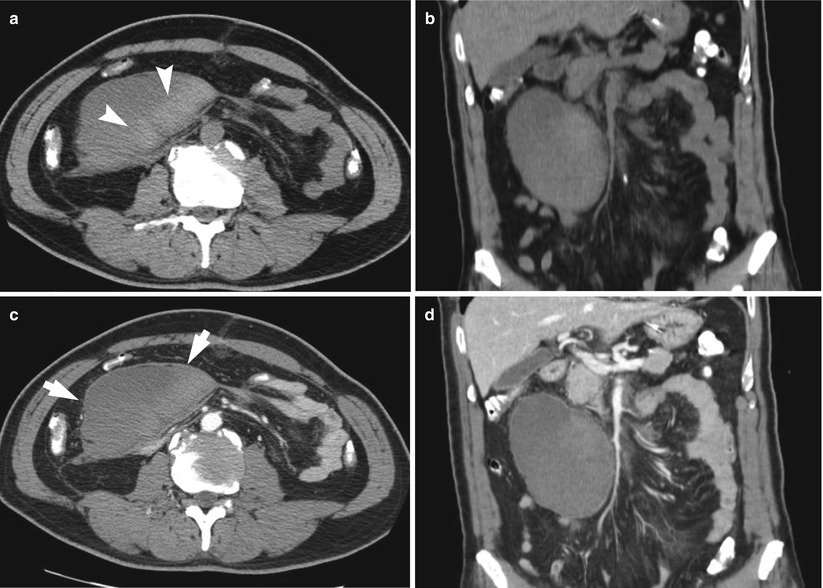
Fig. 21.2
Mesenteric panniculitis. (a, b) Venous phase axial CT images show segmental increased attenuation within the mesenteric fat (arrows) without displacement of the mesenteric vessels and surrounded by a pseudocapsule (arrowheads). (c, d) Venous phase coronal CT images demonstrate segmental, increased attenuation of mesenteric fatty tissue (arrows), and preserved normal fat density around lymph nodes are noted (arrowheads)
21.7.3 Sclerosing Mesenteritis
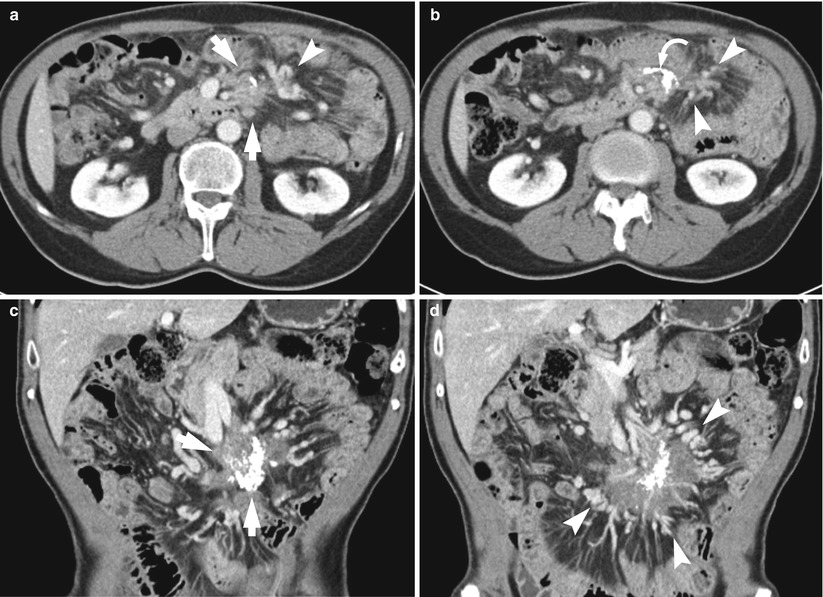
Fig. 21.3
Sclerosing mesenteritis. (a, b) Venous phase axial CT images show ill-defined soft-tissue mass in the mesentery (arrows) with soft-tissue thickening extending into the adjacent fat. The mass is containing calcifications (curved arrow). The tortuous and prominent mesenteric vessels are noted (arrowheads). (c, d) Venous phase coronal CT images demonstrate calcified mass in the mesentery (arrows) with surrounding tortuous mesenteric vessels (arrowheads)
21.7.4 Sclerosing Encapsulating Peritonitis in Patient with Peritoneal Dialysis
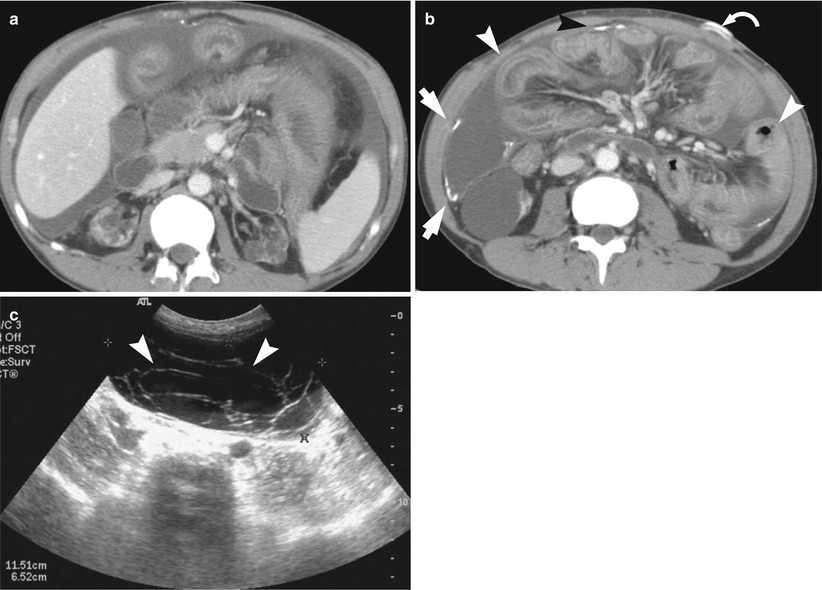
Fig. 21.4
Sclerosing encapsulating peritonitis in patient with peritoneal dialysis. (a, b) Venous phase axial CT images demonstrate calcifications in the peritoneal membranes (arrows), peritoneal thickening, and fluid collections. Small-bowel loops show thickening (arrowheads) and calcification in the bowel wall (black arrowhead). The peritoneal dialysis catheter is noted (curved arrow). (c) Transabdominal US image demonstrates loculate fluid collection in the peritoneal cavity with septations (arrowheads)
21.7.5 Tuberculous Lymphadenopathy
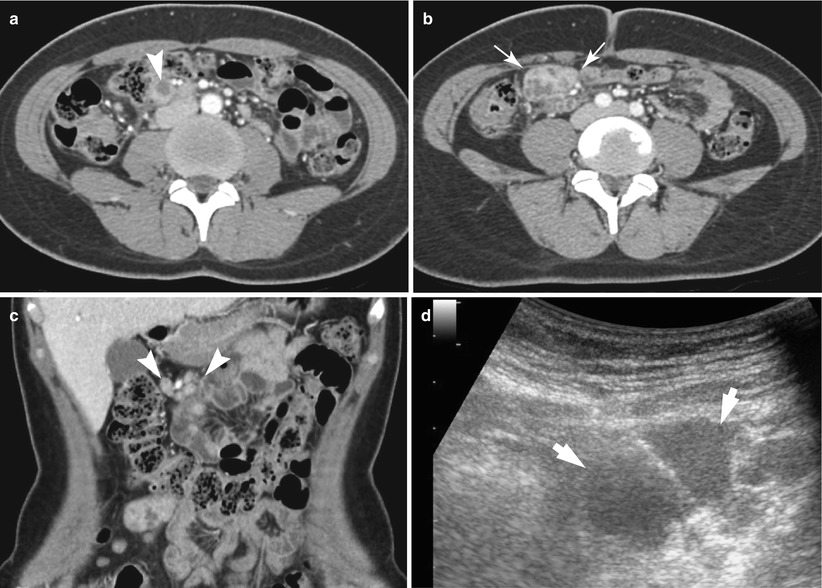
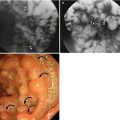
Fig. 21.5
Tuberculous lymphadenopathy. (a, b) Venous phase axial CT images demonstrate enlarged multiple lymph nodes in the mesentery (arrows). A hypodense center is noted (arrowhead). (c) Venous phase coronal CT images show multiple conglomerated lymph nodes in the mesentery (arrowheads). (d) Transabdominal US-guided biopsy was performed. Transabdominal US image demonstrates hypoechoic lymph node in the mesentery (arrows). Tuberculous lymphadenopathy was confirmed
21.7.6 Tuberculous Peritonitis
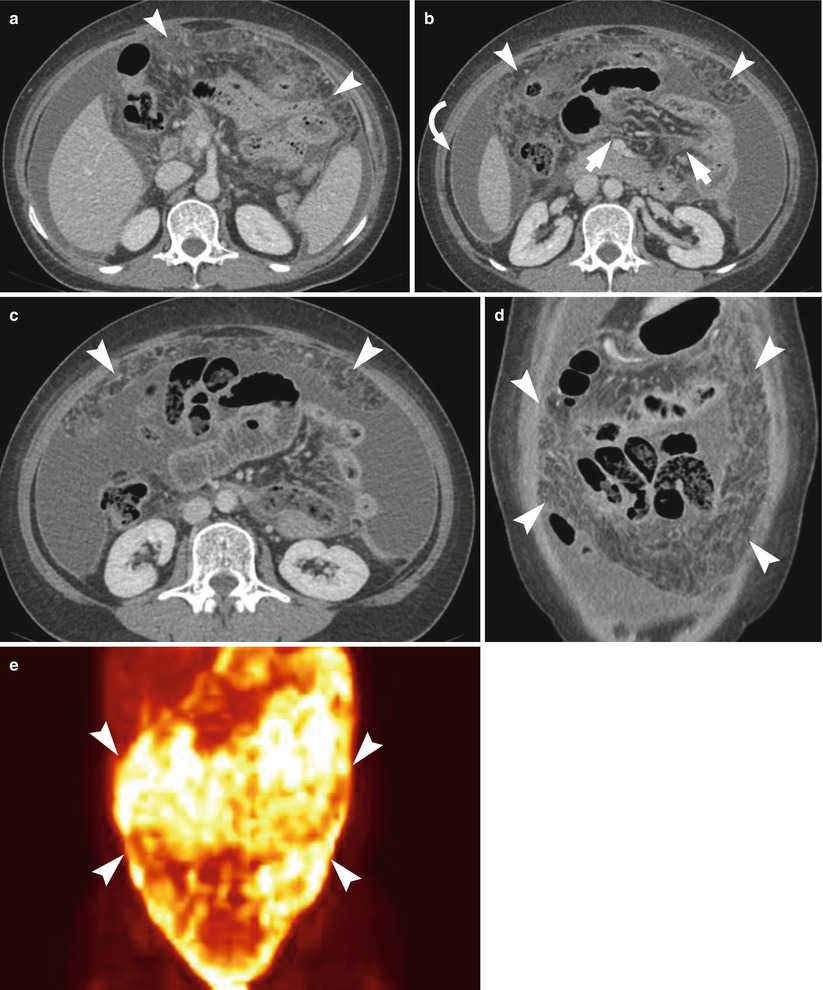
Fig. 21.6
Tuberculous peritonitis. (a–c) Venous phase axial CT images depict large amount of ascites with infiltration in the omentum (arrowheads) and mesentery (arrow). The uniform thickening of the peritoneum is noted (curved arrow). (d) Venous phase coronal CT images show a smudged or dirty appearance of the omentum (arrowheads). (e) FDG-PET scan demonstrates intense FDG uptake in the peritoneum (arrowheads)
21.7.7 Omentum Torsion and Infarction
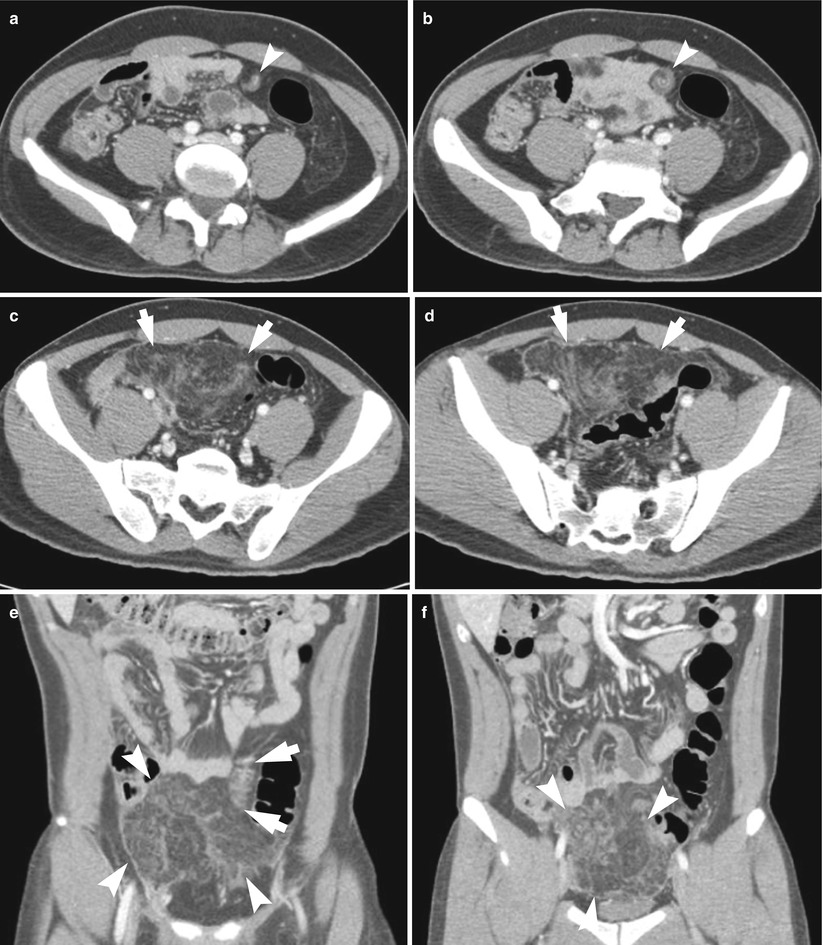
Fig. 21.7
Omentum torsion and infarction. (a–d) Venous phase axial CT images show rotation of the omentum (arrowheads) with oval-shaped streaky infiltration in the distal part of the omentum (arrows). (e, f) Venous phase coronal CT images clearly demonstrate omental torsion (arrows) with interspersed area with streaky infiltration in the distal part of omentum (arrowheads)
21.7.8 Omentum Torsion and Infarction
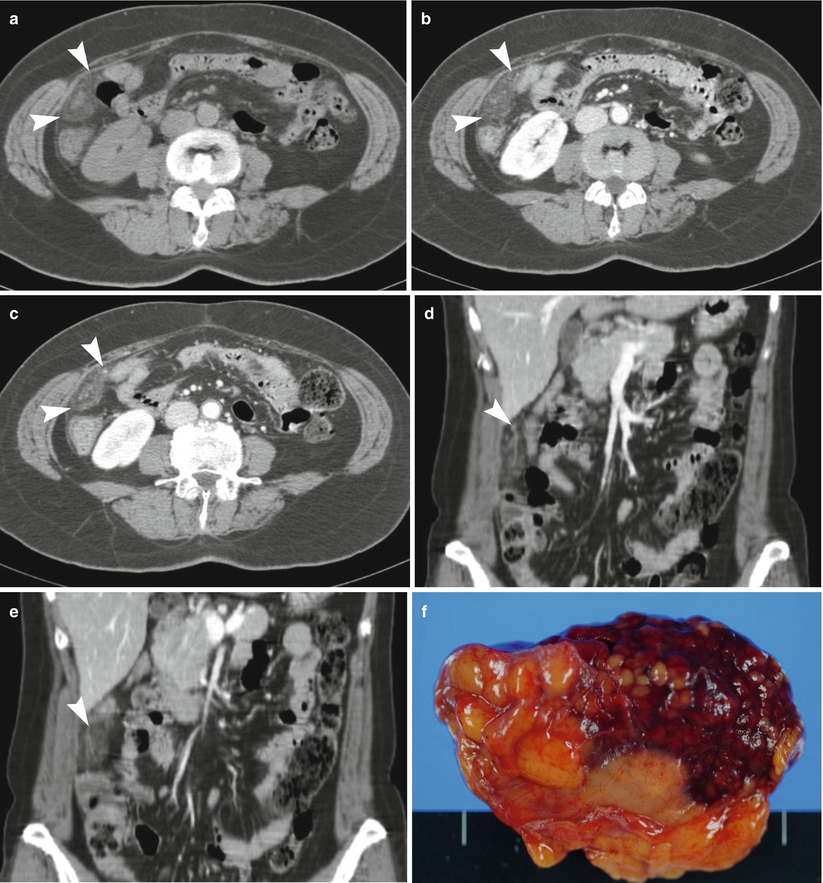
Fig. 21.8
Omentum torsion and infarction (a–c) Venous phase axial CT images demonstrate a triangular-shaped fatty mass in the right side of omentum (arrowheads). (d, e) Venous phase coronal CT images clearly demonstrate streaky infiltration in the right side of omentum with patent branch of omental vessels (arrowheads). (f) Surgical specimen shows fatty mass with hemorrhagic necrosis