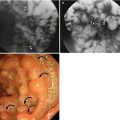
Number of markers in the colon
Right colon
Left colon
Rectosigmoid
Total
4th day
8
9
10
27
7th day
0
0
3
3
8
9
13
30
16.3 Cathartic Colon
Cathartic colon is known to come from chronic use of stimulant/irritant cathartics (e.g., phenolphthalein, cascara, castor oil, senna extract, podophyllum), usually for weight control. Prolonged misusage of stimulant laxatives causes neuromuscular incoordination and deprives colonic musculature of the ability to make adequate contractile force without stimulants; patients cannot achieve proper bowel movement without an assistance of laxatives. Usual symptoms are nonspecific and include abdominal pain, diarrhea, and weight loss; patients initially deny the use of laxatives, and therefore, a wrong medical history leads to an incorrect diagnosis. Previous history of prolonged constipation with laxative usage makes it not so difficult to discriminate these patients from those with inflammatory bowel disease. Radiographic findings include decrease or loss of haustral markings which mimics inflammatory bowel disease, dilatation and spasm of colonic lumen, and pseudostrictures (Bowden et al. 2013). The ileocecal valve frequently becomes patulous.
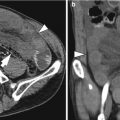
16.4 Sigmoid Volvulus
A volvulus is an obstruction of a bowel loop caused by a twist around its mesenteric attachment. Main predisposing factors for colonic volvulus are redundant mobile colon on a mesocolon and a fixation point around which colonic segment can swirl, and that is why the sigmoid colon is the most frequent site, especially in elder patients. The most common sites for colonic volvulus are as follows: sigmoid colon, 60–75 %; cecum, 25–40 %; and transverse colon, 5–10 % (Peterson et al. 2009). The cause of sigmoid volvulus includes high-fiber diet which produces large bulky stools and resultant dilated and elongated sigmoid colon and chronic constipation and desensitization which can be seen in elderly people in the nursing home or psychological hospitals.
Colonic volvulus often presents a characteristic feature on a plain abdominal radiograph, which may be sufficient for a correct diagnosis in about three-fourth of the patients. Sigmoid volvulus has a typical radiographic appearance of a dilated loop of the sigmoid colon which displays itself as an inverted-U configuration with an absence of haustral marking and the opposed inner walls form a dense white line that runs toward the pelvis, forming a so-called “coffee-bean” sign. As this condition is one of a closed obstruction, there is usually a large amount of gas in the proximal colon and the small intestine. When a correct diagnosis cannot be obtained with plain radiographs, CT may be helpful to make a diagnosis. CT image shows a markedly dilated bowel loop located in the mid to upper abdomen. Swirling mesentery can also be seen at the level of obstruction. As with cases of bowel obstructions in other sites of gastrointestinal tracts, coronal and sagittal reformatted CT images may be useful for evaluating the orientation of rotated bowel segment and exact location of mesenteric swirling.
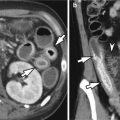
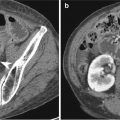
16.5 Colon Intussusception
Among various causes of mechanical obstruction of the intestine in adults, intussusception accounts for 1–3 % and can be categorized into enteroenteric or ileoileal, ileocecal, ileocolic, and colocolic types according to its location and into idiopathic, benign, or malignant according to its cause. With an introduction and wide use of CT as a diagnostic imaging, the chance of incidental detection of intussusception has increased. Most of those patients present no symptom and there is no sign of obstruction. Therefore, treatment or further examination is usually unnecessary.
Demonstrable cause can be found in about 80 % of colonic intussusceptions in adult cases; about half of the colonic intussusception are associated with malignancy, including primary adenocarcinoma, lymphoma, or metastatic disease (Azar and Berger 1997). Other benign causes of intussusception include lipoma, adenomatous polyp, endometriosis, and anastomosis site. Except for the lipoma which is easily noticed on CT as a well-marginated low-attenuating mass, an identification of underlying cause is not easy. Between intussusceptum and intussuscipient, the mesentery (ileocolic) or mesocolon (colocolic) and its vessels invaginate, and the lesions show a “target” sign or a sausage-shaped mass according to the axis of projection.
16.6 Rectocele and Rectal Intussusception
The normal pelvic floor is a complex structure composed of pelvic bones, pelvic floor muscles, and ligaments and provides suspension for intrapelvic organs. They should work properly during urination and defecation. Every activity of lifting, sneezing, laughing, and excretion as well as childbirth of women stresses out pelvic floor structures. Especially for middle-aged multiparous women, pelvic floor weakness is a common problem.
Anterior wall prolapse is a condition in which the anterior wall of the rectum falls down from the normal position because of underlying dysfunction of pelvic floor structures. Rectocele is an outpouching of the rectal wall, usually of which anterior portion protrudes, reflecting relative weakness of the rectovaginal septum. Rectocele is often followed by rectal intussusception, which may interfere defecation. Rectal intussusception is a concentric infolding of the entire rectal wall into the anal canal and may cause rectal prolapse.
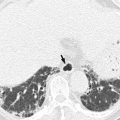
16.7 Pneumatosis Coli
Pneumatosis intestinalis (PI) refers to the presence of gas in the bowel wall; it can be seen in any part of the elementary tract. For the colon, it is called as pneumatosis coli. PI has been traditionally classified into primary and secondary form. The former does not have definite cause and symptom and the latter occurs from gastrointestinal tract infection or necrosis. Pneumatosis cystoides, as one of the primary form, is less common and usually asymptomatic and manifests itself as multiple, thin-walled cysts containing air in the submucosal or subserosal layer mainly in the sigmoid colon and descending colon (Gagliardi et al. 1996). It can mimic polyps as they protrude into the lumen on barium enema or colonoscopy. CT is the best diagnostic tool as it can demonstrate intramural air and surrounding walls. Secondary form is much more common (>80 %) and is associated with various underlying conditions. There are two main theories explaining the mechanism of PI (Gagliardi et al. 1996); first, mechanical theory insists that gas bubbles from the lung or intestinal lumens invaginate into the bowel wall through a small break of the mucosa in the cases of underlying chronic obstructive pulmonary disease (COPD), asthma, mechanical ventilation, or bowel obstruction. Second, bacterial theory insists that gas-forming organisms invade into the bowel wall in the cases of scleroderma, diverticulosis, or immunocompromised states such as bone marrow transplantation or AIDS. An application of nonsteroidal anti-inflammatory drugs for inflammatory bowel disease can be one of the causes. Primary form of PI shows linear and streak-like distribution of intramural airs which run in parallel with the colon wall. On CT scan, the presence of hepatic portal or portomesenteric venous gas should be carefully sought to exclude secondary PI.
16.8 Colonic Pseudo-obstruction
Colonic pseudo-obstruction is a syndrome which mimics mechanical obstruction of the large bowel, but there is no actual cause of obstruction. Because of its uncertain etiology, various names have been designated to this disease entity. They include Ogilvie’s syndrome, pseudomegacolon, adult megacolon, adynamic ileus, and idiopathic large bowel obstruction. It is usually seen in patients with age over 60 associated with poor medical condition such as electrolyte imbalance, systemic infection, trauma, recent surgery, malignancy, medication, or cardiovascular disease. Although there is no actual obstruction point, particularly in its acute form, colonic pseudo-obstruction can evolve to necrosis and perforation of the large bowel. In addition, the colon may dilate up to 12 cm in diameter at the cecum and the risk of perforation increases and colonic decompression should be performed (Choi et al. 2008). CT scan is a single most useful method for the correct diagnosis. A plain abdominal radiography has a limitation as the fluid or fecal content can obscure the margin of colon wall and gives incorrect information for the dilatation of the colon. CT scan shows a prominent dilatation of the colon without distal obstructive lesion. Other useful CT findings include long segmental wall thickening, increased vascularity of marginal vessels, and mucosal fold thickening. Transitional zone can be seen in the splenic flexure or midportion of the transverse colon, and this finding can help in the differentiation of pseudo-obstruction from paralytic ileus. Other diseases which should be considered as a differentiation diagnosis include Hirschsprung’s disease, toxic megacolon, ischemic colitis, fecal impaction with stercoral colitis, and colon cancer.
16.9 Reversed Intestinal Rotation
The chance of intestinal malrotation is approximately one in 6,000 births and most of them present in the neonatal period or early infancy. Manifestation of midgut malrotation in adulthood is extremely rare and usually accompanies with vague abdominal discomfort. Reserved intestinal rotation is one of the rarer conditions; in a literature review, among 192 cases of intestinal malrotation presented in adulthood, 17 cases were reverse rotations (Paci et al. 2013). Patients with reversed intestinal rotation go without symptoms for many years, but eventually develop some kind of intestinal obstruction. This occurs either as a consequence of constriction of the colon as it passes behind the mesenteric vessels or as a consequence of volvulus of the free ileocecal segment. With oral contrast study, a right-sided duodenojejunal junction or proximal jejunal loops highly suggest malrotation. Ultrasonography can demonstrate the reversed position of the superior mesenteric artery (SMA) and superior mesenteric vein (SMV). Duodenal dilatation is another clue for the diagnosis. On CT, the colon is mostly seen in the left and mid abdomen, the small bowel is located in the right abdomen, and the transverse colon runs behind the SMA. A “whirlpool” sign which is composed of SMV around the SMA and torsion of the proximal small bowel can be seen.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


