form an appropriate response to the pathology. Terms for aggressive periostitis include lamellated or “onion skin,” “hair-on-end,” “sunburst,” and Codman’s triangle.4
Table 29.1 PEDIATRIC BONE TUMORS BY PEAK AGE | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 29.2 PEDIATRIC MULTIFOCAL BONE LESIONS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Table 29.3 PEDIATRIC LONG BONE TUMORS BY LOCATION | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
bone (Figs. 29.1 and 29.2). They most often arise from long bone metaphyses and are directed away from the joint. MR is helpful for identifying pathologic fractures and any overlying soft tissue abnormalities.1 On T2W or cartilage-sensitive sequences, the cartilaginous cap is normally a thin crescentic, high-signal structure (Fig. 29.3).
 FIG. 29.1 • Osteochondroma in a 7-year-old male. AP radiograph of the knee shows a pedunculated exostosis arising from the distal femoral metaphysis (arrow). Most osteochondromas are directed away from the adjacent joint, as in this case. |
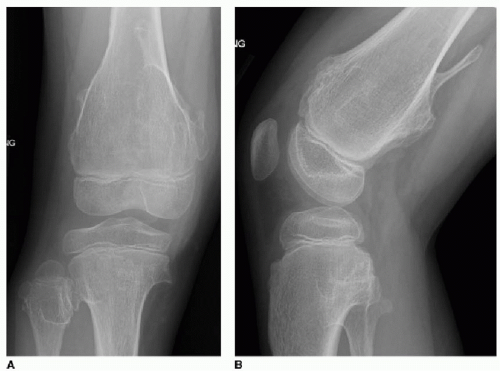 FIG. 29.2 • Multiple hereditary exostoses (MHE) in a 7-year-old female. AP (A) and lateral (B) knee radiographs depict numerous sessile and pedunculated osteochondromas protruding from the distal femur, proximal tibia, and proximal fibula. |
These tumors often present with pain and impaired function of the adjacent joint. Radiographs and CT will show a lobular lucent lesion with sclerotic margins and chondroid calcification, similar to an enchondroma (Fig. 29.7A, B). On MR, there is often surrounding marrow edema and an associated joint effusion (Fig. 29.7C). These peritumoral inflammatory changes are absent with enchondromas. Chondroblastoma is treated with curettage and bone grafting, with a 20% likelihood of local recurrence.1,8, 9 and 10
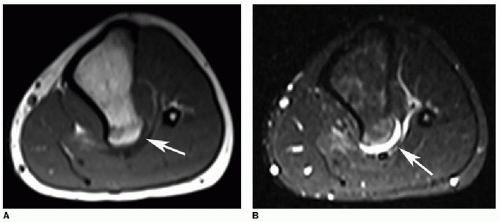 FIG. 29.3 • Osteochondroma in a 16-year-old male. A: Axial T1W image of the left lower leg demonstrates an exostosis arising from the posterior tibia (arrow). Note the marrow continuity between the osteochondroma and the parent bone. B: Axial STIR image shows a thin crescentic, high-signal cartilaginous cap (arrow). |
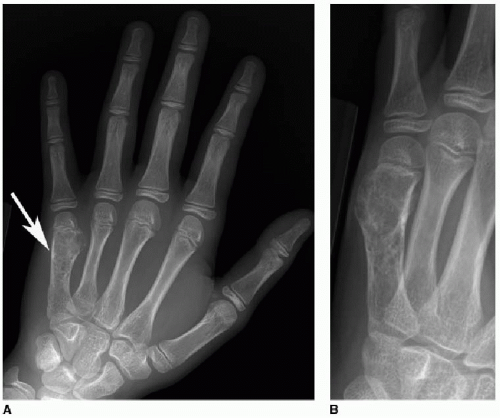 FIG. 29.4 • Enchondroma in a 10-year-old female. Frontal (A) and oblique (B) hand radiographs exhibit an expansile lucent lesion in the fifth metacarpal. Note the “rings and arcs” pattern of calcification within the tumor (B), typical of cartilaginous lesions. Enchondromas are by far the most common primary hand tumor. |
 FIG. 29.5 • Maffucci syndrome in a 14-year-old female. Forearm radiograph demonstrates severe limb deformity caused by numerous enchondromas and soft tissue vascular malformations. Note the dense, “coral-like” calcification in the large enchondromas involving the distal radius and ulna. Calcifications within the soft tissues represent phleboliths associated with venous malformations. All of the long bones are shortened and dysmorphic. |
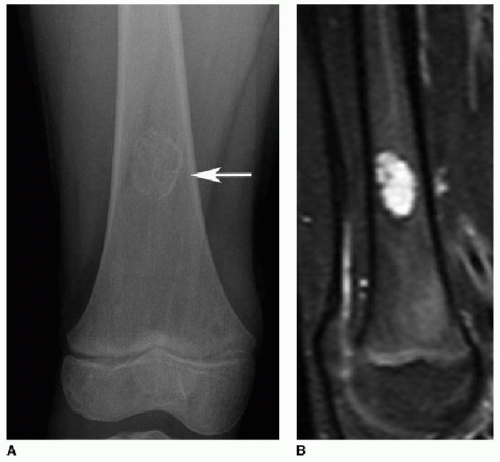 FIG. 29.6 • Enchondroma in a 7-year-old male. A: AP radiograph of the femur exhibits a medullary tumor with a thin sclerotic margin and a “rings and arcs” pattern of internal calcification (arrow). B: Sagittal STIR image shows mostly uniform high signal corresponding to the cartilage. Calcification within and surrounding the tumor is low signal on all sequences. |
bone tumor or vascular malformation. In cases where a pre-existing lesion can be identified, the most common of these is giant cell tumor.12 ABCs are most common in adolescents and young adults and slightly more common in girls. They usually arise in long bone metaphyses and the posterior elements of the spine. Pain and swelling are typical presenting symptoms. As with SBC, treatment for ABC is curettage and bone grafting.1,12,13
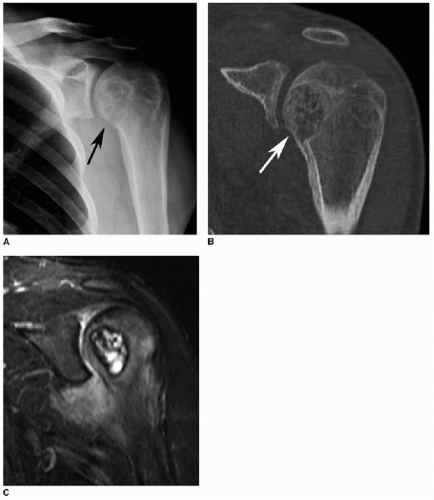 FIG. 29.7 • Chondroblastoma in an 18-year-old male. A,B: AP radiograph (A) and coronal CT image (B) of the left shoulder illustrates a lucent lesion in the humeral head (arrows in A and B). Note the thin sclerotic margin and “rings and arcs” calcification, better characterized on CT. Chondroblastomas are usually located in an epiphysis or apophysis. C: Coronal STIR image shows mixed signal within the lesion—the cartilage is hyperintense, while the calcification is hypointense. There is surrounding marrow edema and a shoulder joint effusion. These inflammatory changes are common with chondroblastomas but absent with enchondromas. |
appear as cortical-based ovoid lucencies with smooth sclerotic margins (Fig. 29.10). They tend to bulge toward the medullary cavity, and the surrounding cortex is intact. As fibroxanthomas involute, they become more sclerotic and less apparent on imaging. Treatment with curettage and bone graft is only indicated for larger lesions at risk for pathologic fracture.7,17, 18, 19 and 20
 FIG. 29.8 • Simple bone cyst (SBC) in a 9-year-old male. AP radiograph of the right humerus exhibits an ovoid lucent lesion with thin sclerotic margins, complicated by a pathologic fracture. The fragments are layering dependently within the cyst, representing the “fallen fragment” sign that is pathognomonic for SBC. |
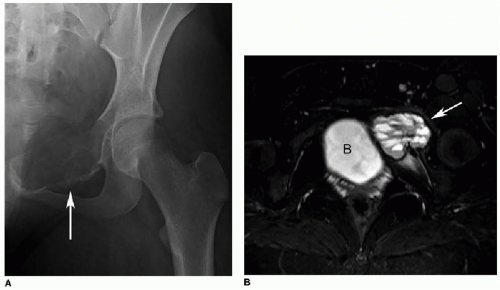 FIG. 29.9 • Aneurysmal bone cyst (ABC) in a 14-year-old female. A: AP pelvis radiograph reveals an expansile lytic lesion in the left superior pubic ramus (arrow). The superior cortex is nearly imperceptible, or “blown-out.” This appearance has been likened to a soap bubble. B: Axial STIR image shows a multiloculated cyst with numerous fluid-fluid levels (arrow). Fluid-fluid levels are typical of ABC but not pathognomonic. (B, bladder.) |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


