1 1.1 Generalized increased bone density 1.2 Solitary sclerotic bone lesion 1.3 Multiple sclerotic bone lesions 2. Osteopoikilosis – asymptomatic. 1–10 mm, round or oval densities in the appendicular skeleton and pelvis. Ribs, skull and spine are usually exempt. Tend to be parallel to the long axis of the affected bones and are especially numerous near the ends of bones. 3. Osteopathia striata (Voorhoeve’s disease) – asymptomatic. Linear bands of dense bone parallel with the long axis of the bone. The appendicular skeleton and pelvis are most frequently affected; skull and clavicles are spared. 1. Metastases (see 1.18) – most commonly prostate or breast. 4. Multiple healed or healing benign or malignant bone lesions – e.g. lytic metastases following radiotherapy or chemotherapy, eosinophilic granuloma and brown tumours. 5. Multiple myeloma* – sclerosis in up to 3% of cases. 6. Osteomata – e.g. Gardner’s syndrome. 1.4 Bone sclerosis with a periosteal reaction 1. Infantile cortical hyperostosis (Caffey’s disease) – in infants up to 6 months of age. Multiple bones involved at different times, most frequently mandible, ribs and clavicles; long bones less commonly; spine, hands and feet are spared. Increased density of bones is caused by massive periosteal new bone. In the long bones the epiphyses and metaphyses are spared. 2. Melorheostosis – cortical and periosteal new bone giving the appearance of molten wax flowing down a burning candle. The hyperostosis tends to extend from one bone to the next. Usually affects one limb but both limbs on one side may be affected. Sometimes it is bilateral but asymmetrical. Skull, spine and ribs are seldom affected. 1.6 Conditions involving skin and bone 1.8 Skeletal metastases – most common radiological appearances 1.11 Lucent bone lesion in the medulla – well-defined, marginal sclerosis, no expansion 1.13 Lucent bone lesion in the medulla – ill-defined Heyning, F. H., Kroon, H. M., Hogendoorn, P. C., et al. MR imaging characteristics in primary lymphoma of bone with emphasis on non-aggressive appearance. Skeletal Radiol. 2007; 36(10):937–944. Nichols, R. E., Dixon, L. B. Radiographic analysis of solitary bone lesions [Review]. Radiol Clin North Am. 2011; 49(6):1095–1114. 1.16 Subarticular lucent bone lesion 1. Osteoarthritis – may be multiple ‘cysts’ in the load-bearing areas of multiple joints. Surrounding sclerotic margin. Joint-space narrowing, subchondral sclerosis and osteophytes. 2. Rheumatoid arthritis* – no sclerotic margin. Begins periarticularly near the insertion of the joint capsule. Joint-space narrowing and juxta-articular osteoporosis. 3. Calcium pyrophosphate arthropathy (see Calcium pyrophosphate dihydrate deposition disease*) – similar to osteoarthritis but frequently larger and with more collapse and fragmentation of the articular surface. 4. Gout – ± erosions with overhanging edges and adjacent soft-tissue masses.
Bones
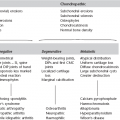
Neoplastic
Developmental
Neoplastic
Idiopathic


Arthritides
Bones