12 Carcinoma Breast cancer is the most common malignant disease in women worldwide, with high prevalence in North America and Europe, with approximately 180 000 invasive and 62 000 in situ breast carcinomas expected to be diagnosed in the United States in 2007. The death rate has declined annually since 1990, with a 3.3% per year decrease in the death rate of women under the age of 50 years and 2.0% per year for women over 50 years. The incidence of breast cancer increases with age; the two greatest risk factors are being female and aging, with the steepest increase occurring before age 50, with increase in incidence continuing but leveling off after 50. About 25% of breast cancer patients are premenopausal, and young age should not be considered as breast cancer protection in young women, especially when imaging findings are indeterminate. Nearly half of diagnosed carcinomas (48%) occur in the upper outer quadrant of the breast (Table 12.1), site of the greatest concentration of breast fibroglandular tissue, but all areas should be carefully examined because inner-quadrant tumors and peripheral lesions close to the chest wall are easily overlooked or else may not be included on poorly positioned mammograms. Tumor size and the presence of multiple foci in one breast are of major importance in surgical planning. Several foci occurring in the same breast quadrant or separated by less than 4–5cm are described as “multifocal,” and several lesions in different breast quadrants or separated by more than 5 cm are classified as multicentric. If other eligibility requirements for breast conservation are met, lumpectomy may be planned for multifocal invasive or intraductal carcinoma. The incidence of multifocal carcinoma ranges from 20% to 40% in different published series. These statistics are difficult to obtain, and perhaps the growing utilization of contrast-enhanced MRI for preoperative evaluation of extent of disease in newly diagnosed breast cancer patients will shed light on an important consideration in treatment planning. Some of the many different types of breast carcinoma are listed in Table 12.2. The tumors are classified by their tissue sites of origin, for the most part either ductal or lobular, and these are divided into further subtypes according to their pattern of growth. Carcinomas are also classified as invasive or noninvasive. Additionally there are several types of rare malignancy, and some lesions are metastatic from primary tumors in other organs. The early detection of breast cancer is important in terms of providing effective treatment, and the decrease in mortality in the last 25 years, is due to earlier detection by mammography and to better treatment, which also may be enabled by more widespread use of mammography and perhaps to improved or new adjunctive methods of screening.
Clinical Significance
Site of occurrence | Frequency (%) |
Upper outer quadrant | 48 |
Upper inner quadrant | 15 |
Lower outer quadrant | 11 |
Lower inner quadrant | 6 |
Central (subareolar) | 17 |
Type of carcinoma | Percentage incidence |
Invasive ductal carcinoma | 75% |
Scirrhous Solid Adenomatous |
|
Invasive lobular carcinoma | 15% |
Special forms | 10% |
Inflammatory Apocrine Mucinous Medullary Tubular Sarcoma Lymphoma Paget disease Squamous cell carcinoma Metastases from other organs |
|
Noninvasive carcinomas |
|
Ductal carcinoma in situ (DCIS) Comedocarcinoma Lobular carcinoma in situ (LCIS) |
|
The doubling time of breast cancers is highly variable, although many grow very slowly. Ten or more years may elapse between carcinogenesis and the initial appearance of clinical manifestations. Some tumors grow much more rapidly than this, but others grow even more slowly. Besides tumor size, the lymph node status, tumor grade, and receptor status have been identified as important prognostic factors along with an increasing number of other prognostic factors, which are the subject of continuing scientific investigation.
Diagnostic Criteria
Carcinomas can have a wide variety of sonographic features. Detectability and characterization depend on technical quality of the equipment and the image produced—contrast and spatial resolution, gray scale, field of view, dynamic range—as well as recognition within the small window of the scan of subtle abnormalities such as architectural distortion that may indicate presence of tumor. As with mammography, where a white tumor is unseen against the background of white fibroglandular tissue, lack of contrast may limit perception of a mass with ultrasound. Fibroadenomas, hypoechoic and oval, may be difficult to impossible to identify when they are in a background of fat lobules, also hypoechoic and oval; malignant tumors, also hypoechoic, often grow within the fibroglandular layer and are conspicuous as dark (hypoechoic) masses standing out in contrast with the light gray fibroglandular tissue (Figs. 12.1–12.3 a, b). It is important to take these factors into account when interpreting ultrasound findings.
Typical Findings
Shape and Margins
As in mammography, a typical malignant tumor appears sonographically as a mass of variably irregular shape with margins that are not circumscribed. Within the category of masses that are not circumscribed, a lesion may exhibit any or all of the following marginal characteristics: indistinctness, angularity, microlobulation, and spiculation (Figs. 12.4a, b–12.6a, b, Table 12.3). Variable compression of the transducer on the breast is useful technique for evaluating the tumor’s shape and its margins.
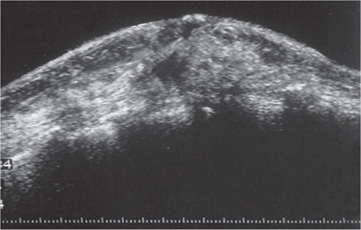
Fig. 12.1 Water-bath immersion scan of an invasive carcinoma 2 cm in diameter.
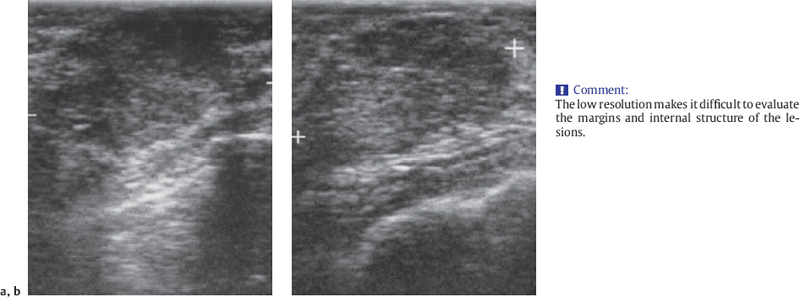
Fig. 12.2 a, b Benign–malignant differentiation is difficult to accomplish with a simple 5-MHz linear-array transducer. a Invasive ductal carcinoma 5 cm in diameter. b Fibroadenoma 4.7 cm in diameter.
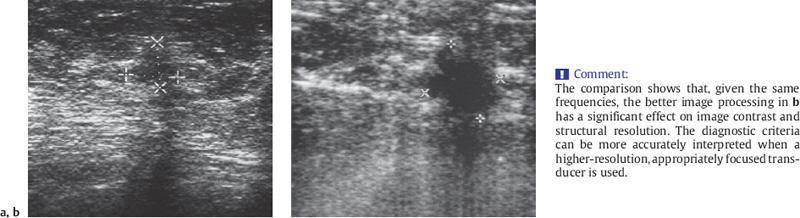
Fig. 12.3 a, b Comparison of a short-focused and b high-resolution 5-MHz transducers, shown here for an invasive ductal carcinoma 1.8 cm in diameter.
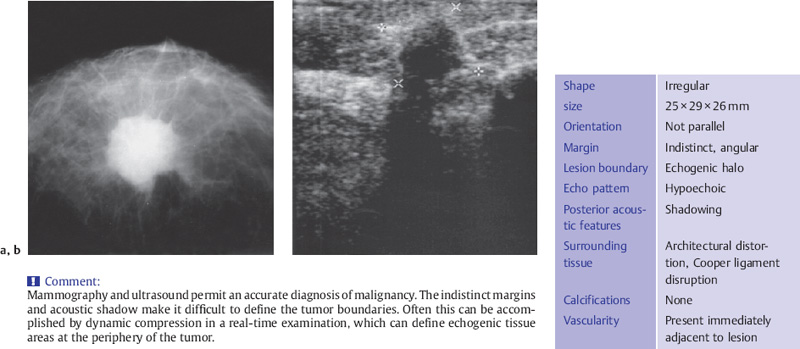
Fig. 12.4 a, b Example of an invasive ductal breast carcinoma.
a X-ray mammography.
b Ultrasound (7.5 MHz transducer).
Echogenicity
The echogenicity of many invasive ductal carcinomas is often heterogeneously hypoechoic and, at least in invasive ductal carcinoma, is usually hypoechoic. Malignant tumors can vary widely in their echo characteristics, however, ranging from nearly anechoic to almost entirely hyperechoic, although in real-time scanning through echogenic carcinomas, one can almost always discern at least a small hypoechoic component (Figs. 12.4 a, b–12.7 a, b).
Shape | Irregular |
Orientation | Not parallel |
Margin | Indistinct (angular, microlobulated, spiculated) |
Lesion boundary | Echogenic halo |
Echo pattern | Hypoechoic, inhomogeneous |
Posterior acoustic features | Shadowing |
Surrounding tissue | Architectural distortion: – Duct changes (irregularities, dilatation) – Cooper ligament changes (disruption, retraction) – Skin thickening, retraction, irregularity |
Calcifications | Microcalcifications in mass |
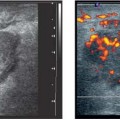
Vascularity | Present in lesion and/or immediately adjacent to lesion |
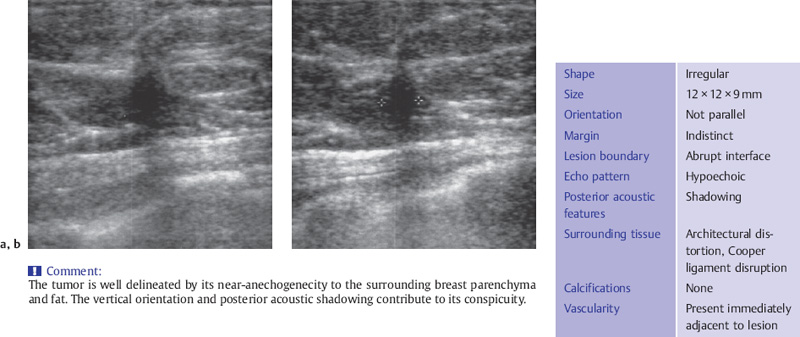
Fig. 12.5 a, b Typical appearance of invasive ductal carcinoma.
a Sagittal scan.
b Transverse scan (10 MHz transducer).
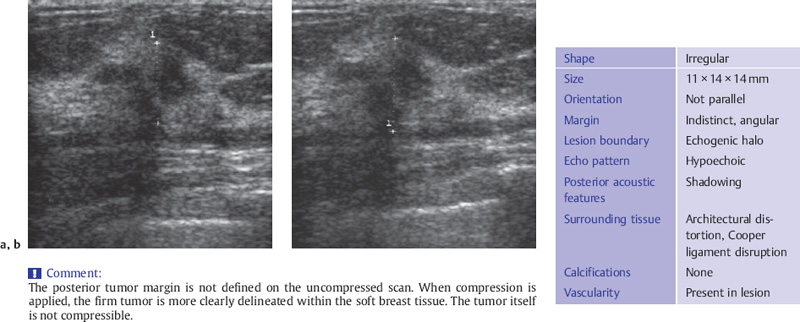
Fig. 12.6 a, b Invasive ductal carcinoma.
a Without compression.
b With compression.
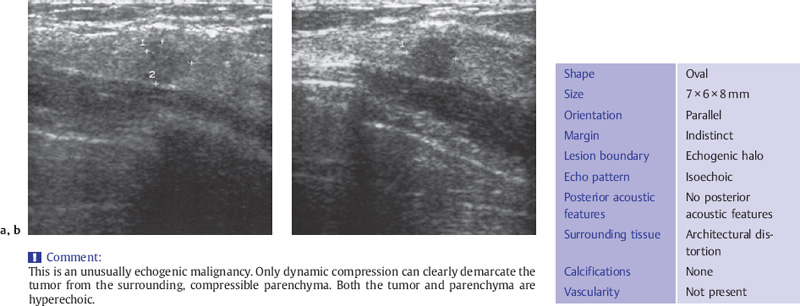
Fig. 12.7 a, b Isoechoic invasive ductal carcinoma.
a Sagittal scan.
b Transverse scan.
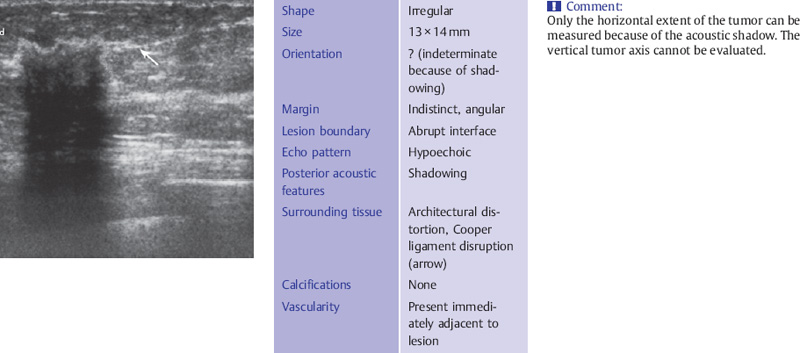
Fig. 12.8 Invasive ductal carcinoma with a strong acoustic shadow.
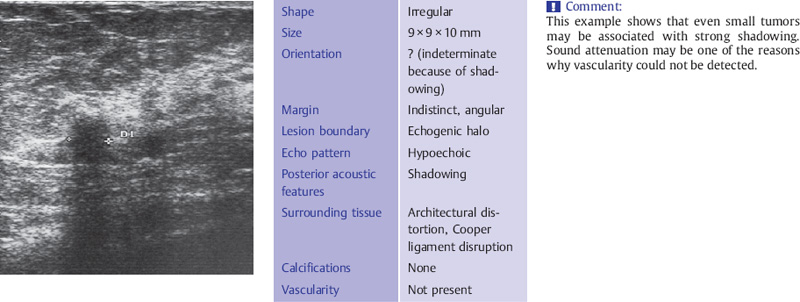
Fig. 12.9 Invasive ductal carcinoma with shadowing.
Posterior Features
Approximately 60% of carcinomas cast acoustic shadows for several reasons. Desmoplasia, a fibrous stromal response to a tumor’s presence, is strongly attenuating. Posterior acoustic shadowing may be sufficiently intense to completely obscure the breast tissue deep to the carcinoma. Marginal spicules may also be associated with this fibrous response associated with some lower-grade (1 and 2) invasive ductal carcinomas. A favorable prognosis has been associated with this sonographic pattern. Their heterogeneity also has an attenuating effect on sound through-transmission (Figs. 12.8, 12.9). Absence of shadowing is not a reliable criterion, however. Approximately 40% of carcinomas are relatively cellular and either elicit no change in acoustic attenuation or enhance posteriorly (Figs. 12.10, 12.11). In general, these are higher grade, less well differentiated neoplasms that have a blander ultrasound appearance related to lack of fibrotic response.
Orientation
Another criterion for malignancy is the orientation of the tumor with respect to the skin; that is, whether its long axis is parallel to the skin (synonyms: horizontal, wider-than-tall) or perpendicular (orientation not parallel to the skin, taller-than-wide). If the horizontal extent of the tumor is greater than its vertical extent and the lesion is circumscribed and no malignant features are present, the lesion is benign or probably benign. A predominantly vertical orientation is more suggestive of malignancy (Figs. 12.12, 12.13).
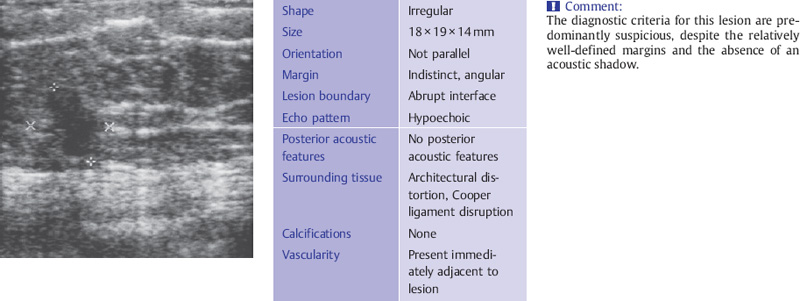
Fig. 12.10 Nonattenuating invasive ductal carcinoma.
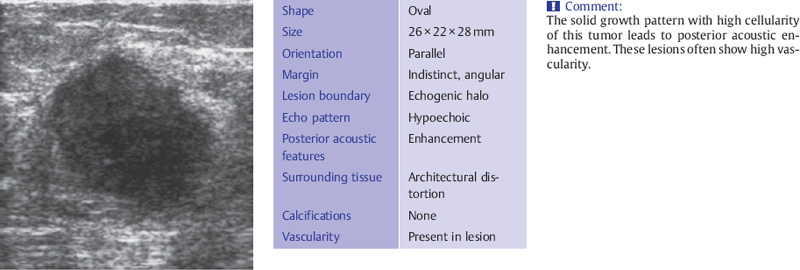
Fig. 12.11 Solid invasive ductal carcinoma with posterior enhancement.
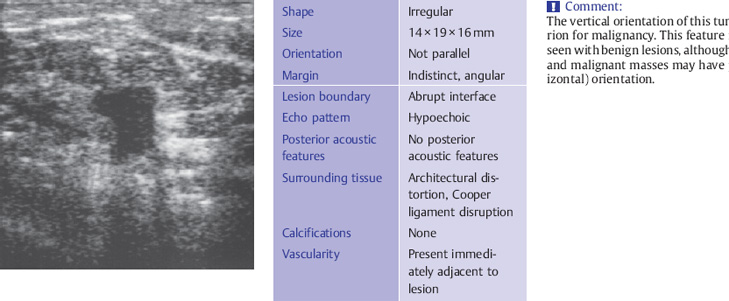
Fig. 12.12 Invasive ductal carcinoma with vertical tumor axis.
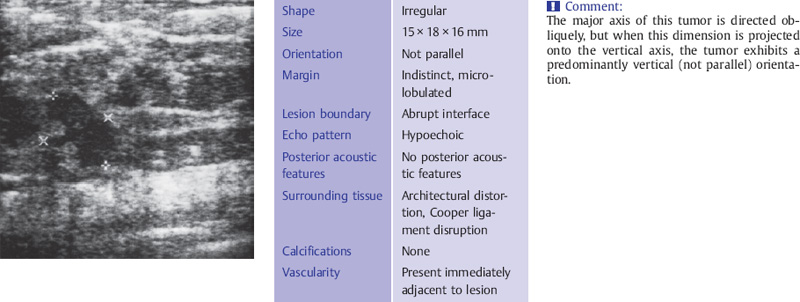
Fig. 12.13 Invasive ductal carcinoma with an oblique tumor axis.
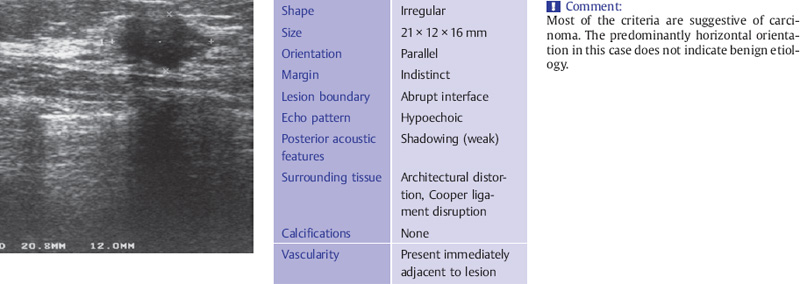
Fig. 12.14 Invasive ductal carcinoma with a horizontal tumor axis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


