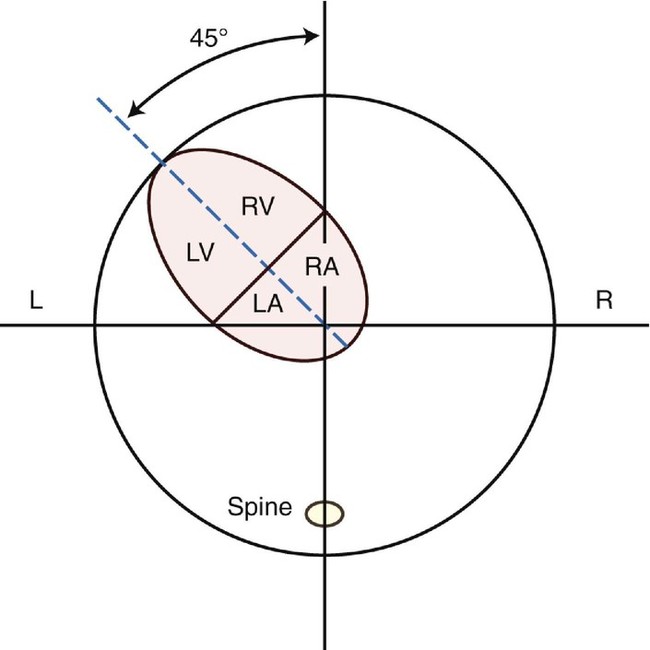
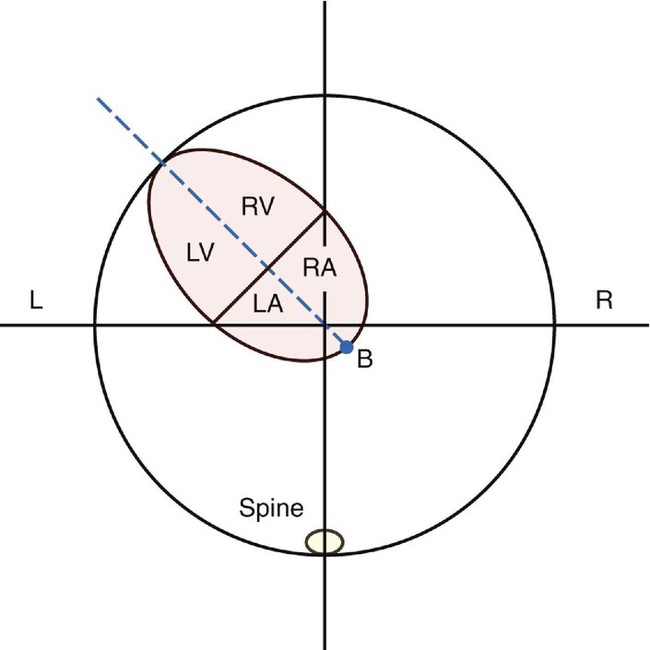
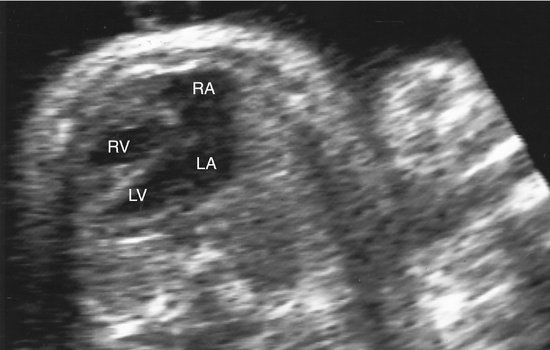
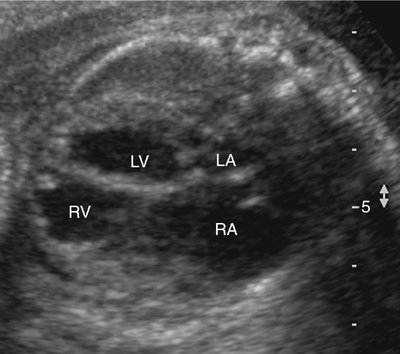
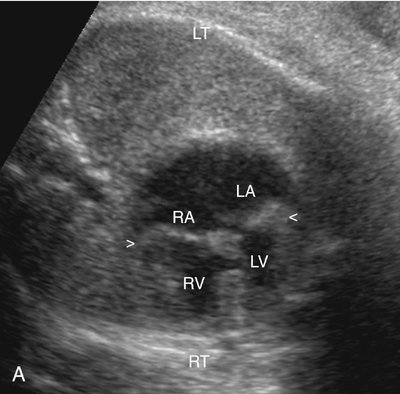
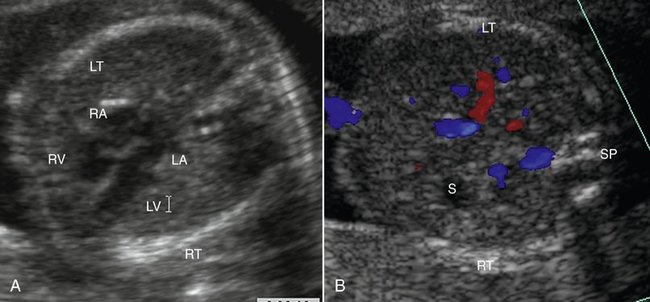
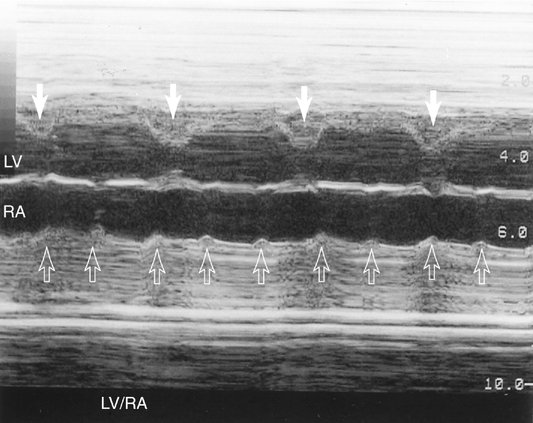
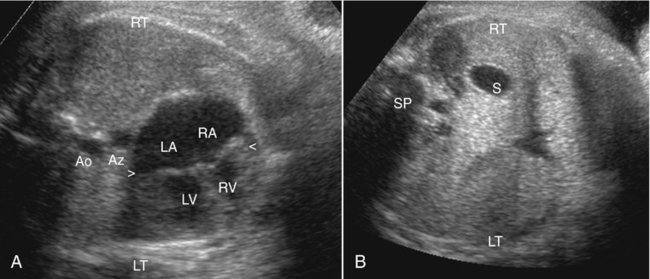
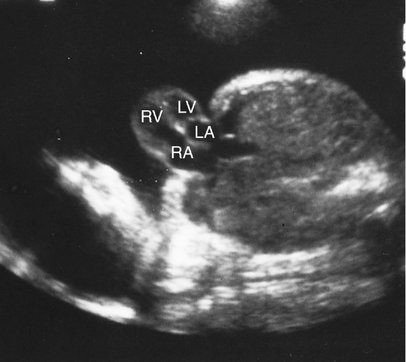
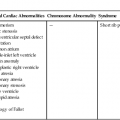
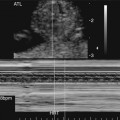
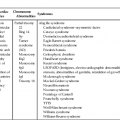
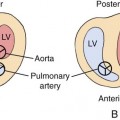
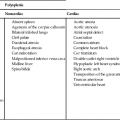
CHAPTER 3 Paul D. Russ and Julia A. Drose Axis and position are two basic morphological features of the fetal heart.1–4 Axis describes the rotational orientation of the heart in the thorax.l–3 It refers to the degree that the cardiac apex points to the left or right. Position describes the translational relationship or overall location of the heart in the chest.1,3,4 It indicates the hemithorax that the heart predominantly occupies. Many anomalies alter either the cardiac axis or the cardiac position. In general, abnormal axis is a manifestation of intrinsic congenital heart disease (CHD), whereas altered position results from an extracardiac defect. Both axis and position can be readily evaluated with the four-chamber view during either routine obstetrical ultrasonography or formal fetal echocardiography.1–4 Cardiac axis can be considered in two ways. Axis can be measured as the angle between a line along the interventricular septum and an anteroposterior line that bisects the thorax (Fig. 3–1).1 This defines the rotational orientation of the heart with respect to the chest wall. In normal fetuses, this angle is about 45 degrees, plus or minus 20 degrees, leftward of midline.1–4 This does not change significantly during gestation.2 Another aspect of axis is the comparison of the heart’s orientation to the location of other organs, particularly those of the upper abdomen. For example, the cardiac apex normally points toward the stomach on the left side of the fetus.4 Cardiac position can be described by a line extending along the interatrial septum (Fig. 3–2). A point is defined at its intersection with the posterior margin of the heart.1 This point is relatively independent of axis and normally is just to the right of midline, close to the center of the thorax. Expressed more simply, most of the fetal heart, especially the ventricles, is positioned in the left anterior quadrant of the chest.1 The right ventricle is normally near the left anterior chest wall, and the left atrium is anterior to the descending aorta and spine.5 Abnormal axis is often associated with complex intracardiac defects and sometimes with intractable arrhythmias. Because the structural abnormalities can be complicated, a systematic or segmental evaluation of the heart is recommended.4–6 Such an evaluation includes determining venoatrial, atrioventricular (AV), and ventriculoarterial (VA) connections.4,6 The segmental approach also establishes the relationship of the heart chambers and cardiac axis to the arrangement of other intrathoracic and abdominal organs. This description of body configuration is defined in terms of situs.4–11 Although the terminology is variable and sometimes confusing, abnormalities of cardiac axis can be generally categorized as dextrocardia, mesocardia, and severe levocardia.6–12 With dextrocardia, the cardiac apex points to the right. If mesocardia is present, the apex is in a midline position. With severe levocardia, it is directed further leftward than the angle previously described.1,6,11 There are three types of situs: situs solitus, situs inversus, and situs ambiguous.4,8,11 Situs solitus is the normal organ arrangement, which includes the liver on the right side and the stomach on the left side. With situs inversus, there is a mirror-image configuration so that the liver is on the left and the stomach is on the right. If there is neither situs solitus nor situs inversus, there is situs ambiguous, also referred to as indeterminate situs or heterotaxy.7,8,10,11 The terms atrial or visceroatrial situs are often used in discussions of situs solitus, situs inversus, and situs ambiguous.4,6,8,10–12 These modifiers emphasize the anatomical interrelationship of atrial and upper abdominal organ arrangement. Although there are exceptions, atrial and visceral situs are usually concordant in situs solitus or situs inversus4,6,8,10,11; that is, the morphological right atrium is located on the same side as the liver. This reflects the fact that the systemic venous connections to the right atrium tend to be the most anatomically constant.7 In bilateral right-sidedness and bilateral left-sidedness, the two major subtypes of situs ambiguous, visceroatrial situs has a different but consistent pattern. With bilateral right-sidedness (asplenia syndrome), both atria have the morphological features of right atria. When there is bilateral left-sidedness (polysplenia syndrome), both atria have the morphological characteristics of left atria.4–6,8,10,11 The likelihood and type of CHD can be predicted by evaluating the cardiac axis as a function of situs.6–11 For each situs-axis pair, several permutations are possible if AV and VA connections are considered.6–10 Anomalous AV anatomy is usually manifested as ventricular inversion; the ventricles are switched so that the right atrium drains into the morphological left ventricle and the left atrium drains into the morphological right ventricle.6,7,9 Abnormal or discordant VA connections correspond to transposition of the great vessels; the aorta arises from the anatomical right ventricle and the pulmonary artery arises from the left ventricle.4,6–8,10 In corrected transposition, there is ventricular inversion with transposition of the great vessels.6–9 Fetal echocardiography is facilitated by considering the more common combinations of axis, situs, and AV and VA connections. Situs solitus with levocardia is the normal body configuration (Fig. 3–3). It is associated with CHD in fewer than 1% of cases.11 However, an extreme leftward axis deviation or levorotation (severe levocardia) of greater than 57 to 75 degrees correlates with a significantly increased risk of a heart defect (Fig. 3–4).2,3 Abnormalities that can have pronounced levorotation include truncus arteriosus, Ebstein anomaly, pulmonary stenosis, coarctation of the aorta, tetralogy of Fallot (TOF), transposition of the great arteries, and double-outlet right ventricle (DORV). Because of the frequent conotruncal and great vessel defects, the echocardiographic examination should be more extensive than the four-chamber view alone.2,3 The reason that CHD occurs with extreme levorotation in situs solitus is not known. Abnormal chamber size, for example, the enlarged right atrium in Ebstein anomaly, could cause the leftward axis deviation (Fig. 3–5).2 It is also postulated that defective hearts overrotate from right to left during embryogenesis.2,3 Extracardiac anomalies such as omphalocele, hydrocephalus, Dandy-Walker malformation, diaphragmatic hernia, and renal agenesis can be present. Abnormal karyotypes are not infrequent and include trisomy 21, trisomy 18, and trisomy 13.2,3 Situs solitus with dextrocardia is also referred to as dextroversion or isolated dextrocardia (Fig. 3–6, A and B).6–8 This condition is found in 1 in 29,000 individuals in the general population. It is associated with CHD in 95% of cases.11 Situs solitus with dextrocardia can be divided into two subgroups. In one type, the AV and VA relationships are usually normal.6,8–10 Sometimes there is complete transposition of the great arteries.8 There are often other abnormalities such as atrial septal defect (ASD), ventricular septal defect (VSD), atrioventricular septal defect (AVSD), coarctation of the aorta, and anomalous pulmonary venous connections.6 This dextroversion can be complicated by an ectopia cordis variant, namely, herniation of a left ventricular diverticulum through the anterior diaphragm into the epigastrium.8 The other type of situs solitus with dextrocardia is associated with both AV and VA discordance or corrected transposition. Corrected transposition is common in dextroversion, occurring in up to 90% of cases.6,7,10 This type of situs solitus is often also complicated by VSD and pulmonary stenosis.6,8 Other abnormalities that can be present include AVSD, TOF, pulmonary atresia, Ebstein anomaly, and anomalous systemic and pulmonary venous connections.6,7 Situs inversus is rare. It occurs in about 0.00005% of patients.11 In most cases of situs inversus, the atrial and visceral situs are concordant; that is, there is dextrocardia.8,11 Occasionally, the cardiac apex points leftward in situs inversus, a condition termed levoversion or isolated levocardia.6–9,11 Situs inversus with dextrocardia is referred to as mirror-image dextrocardia (Fig. 3–7, A and B).6–11 Although the right atrium and right ventricle are on the left side and the left atrium and left ventricle are on the right side, there are usually physiological AV and VA connections.6,7,9 Consequently, CHD is not common. Associated cardiac defects are found in 0.3% to 5% of patients.7,11 Abnormalities that occur include ASD, VSD, AVSD, pulmonary atresia, TOF, and DORV.6,10 If there is VA or AV plus VA discordance, the mirror-image equivalent of complete transposition or corrected transposition, respectively, is found.6,10 Situs inversus with levoversion or isolated levocardia is extremely rare.11 It is the mirror-image of situs solitus with dextroversion.8 CHD occurs in almost 100% of cases.11 The inverted equivalent of corrected transposition is common.6,8,10 There is also an association with DORV.6,10 Systemic venous anomalies such as the lack of an inferior vena cava can be present.9 Mesocardia is uncommon (Fig. 3–8).6 In one study, only 17 cases were noted among 3150 patients with CHD.12 In another series that was based on a registry of about 3000 specimens, only seven of 65 malpositioned hearts manifested mesocardia.10 The low frequency of mesocardia could be artificial because cases tend to be grouped according to either dextroversion or levoversion.6 For example, in situs solitus, mesocardia reflects incomplete dextroversion.6–9,12 In situs inversus, a heart in the midline corresponds to partial levoversion.6,12 Mesocardia occurs with situs solitus, situs inversus, and situs ambiguous.6,10,12 As expected, the cardiac defects in mesocardia resemble those found in dextroversion and levoversion.6 Many cases are associated with corrected transposition and complete transposition.6,7,10,12 Other abnormalities that can be found include DORV, a single ventricle, AVSD, and pulmonary stenosis or pulmonary atresia.10,12 Situs ambiguous is associated with two distinct syndromes: asplenia and polysplenia.11 The visceroatrial situs in both is unusual. In asplenia or Ivemark syndrome, there is right atrial isomerism and bilateral right-sidedness.* Both atria have symmetrical right atrial morphological features.11 Each lung is trilobed with an epiarterial bronchus.8 The liver is often in a midline position, and the spleen is absent.11,14 The stomach can be in the midepigastrium or located to either side of the abdomen.11 In polysplenia syndrome, there is left atrial isomerism and bilateral left-sidedness.6,8,11,14 Both atria have features of the left atrium.8 The lungs are bilobed with hyparterial bronchi.11 In polysplenia, the abdominal organs tend to be less symmetrical than is the case in asplenia.10 The liver is in a midline position in about one half of patients.8 Multiple clumped splenules are usually unilateral and are located along the greater curvature of the stomach.6,8,11 In up to 60% of patients, the position of the stomach is either in the midline or to the left.14 Asplenia syndrome is associated with CHD in 99% to 100% of patients.11 Dextrocardia, mesocardia, and levocardia can occur.6,11 The cardiac anomalies in asplenia syndrome tend to be more severe than those in polysplenia syndrome.11 There is often corrected or complete transposition of the great arteries.6,8,10 ASD and AVSD are common.6,8,10,11 There is a single ventricle in 50% of individuals and pulmonary stenosis or atresia in 75%.8 Total anomalous pulmonary venous connection, particularly with return to the portal vein, often occurs.8 Systemic venous abnormalities include bilateral superior venae cavae.6,8,10 There is a lower incidence of CHD in polysplenia syndrome. About 5% to 10% of patients have no heart disease. Associated cardiac defects tend to be milder compared with those of asplenia syndrome.11 In polysplenia syndrome, the cardiac apex is rotated rightward in about 50% of cases and otherwise points to the left.8,10 Mesocardia is uncommon.10,15 Transposition of the great arteries is less frequent than in asplenia syndrome.10 Although complete or corrected transposition can occur, the aorta–pulmonary arterial interrelationship is normal in 70% of patients. ASD, VSD, and AVSD are common.8,10 A single ventricle is present in only 5% of hearts, but DORV is found in about 30%.10 In contrast to asplenia syndrome, pulmonary stenosis or atresia is absent in two thirds of patients.6–8,10 However, 40% to 50% of patients have left-sided obstructive lesions such as coarctation of the aorta, aortic stenosis, left ventricular hypoplasia, and mitral stenosis.8,11 An anomalous pulmonary venous connection is common, but it is usually partial rather than total.10 A characteristic feature of polysplenia is interruption of the hepatic portion of the inferior vena cava with azygous or hemiazygous continuation.8,10,11,14 This condition occurs in about two thirds of patients.8,14 Complete heart block with bradycardia is common in polysplenia syndrome (Fig. 3–9).4,5,11,14–16 It is often associated with an AVSD (Fig. 3–10).4,5,14–16 AV block is apparently related to malformation and degeneration of the conduction system in these hearts.15–17 Polysplenia syndrome has been detected and diagnosed prenatally with ultrasound.4,5,14,16,18 Nonimmune hydrops fetalis, the stomach on the right side, an interrupted inferior vena cava with azygous continuation, AVSD, and complete heart block have been demonstrated (see Figs. 3–9 and 3–10, A and B). The prognosis for fetuses with left atrial isomerism, complete AV block, and AVSD is poor. In utero and neonatal mortality rates are high.5,14–16 As previously noted, fetal heart position can be defined separately from cardiac axis.1 An abnormal position often indicates the presence of congenital defects that are different from those associated with an axis deviation. This distinction is emphasized by using the terms “dextroposition” and “levoposition” to describe the pathological displacement of the heart into the right or left thorax, respectively.1,3,8,10,11 Extracardiac malformations are common and are often responsible for the abnormal location of the heart. In essence, the extracardiac defect pushes the heart out of its more midline location. These malformations include thoracoabdominal wall and diaphragmatic defects, a variety of pulmonary lesions, pleural disease, and miscellaneous intrathoracic tumors. Ectopia cordis represents partial or complete displacement of the heart from the thoracic cavity.6 It can be classified into five types according to heart location: cervical, thoracocervical, thoracic, thoracoabdominal, and abdominal.6,19,20 In the cervical form, the heart is in the neck and the sternum is intact. In the thoracocervical type, the heart protrudes through a defect in the superior sternum.6,20 In thoracic ectopia cordis, there is a sternal defect and the heart lies outside the chest wall.20,21 The thoracoabdominal type is associated with a common defect of the ventral lower thorax and midepigastrium (Fig. 3–11). In the abdominal form of ectopia cordis, a diaphragmatic gap allows the heart to enter the upper abdomen (Fig. 3–12).6,20,21 The thoracoabdominal type accounts for 7% of cases.19,21 This malformation complex is known as the pentalogy of Cantrell (see Fig. 3–11).19 In its complete form, ectopia cordis is associated with a deficient anterior pericardium, an inferior sternal defect, a ventral diaphragmatic opening, a supraumbilical abdominal wall defect (usually omphalocele), and congenital heart anomalies.19,22–28 Pentalogy of Cantrell variants have been reported.19,27 Some patients manifest three major features, including diaphragmatic, abdominal wall, and intracardiac defects.19
Cardiac Malposition
Abnormal Cardiac Axis
Abdominal Situs
Situs Solitus
Situs Inversus
Situs Ambiguous
Abnormal Cardiac Position
Ectopia Cordis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Cardiac Malposition