CHAPTER 19
Cardiosplenic Syndromes
Definition
Visceral heterotaxy represents approximately 30% of cardiac malpositions in infants and 45% of the deaths associated with these conditions.1
Asplenia is characterized by bilateral right sidedness or right atrial isomerism. Typical features of this syndrome include bilateral right atrial appendages, bilateral morphological right lungs (trilobed), an absent spleen, a midline liver, and multiple cardiac anomalies.2–6 The stomach, liver, and gallbladder are likely to be in a situs ambiguous or inversus position.7 A malpositioned inferior vena cava, which may be anterior or juxtaposed to the aorta, and abnormal pulmonary venous return are frequently seen.2,8,9
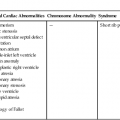
The incidence of cardiac abnormalities associated with asplenia is high. Atrioventricular septal defects are reported in approximately 85% to 95% of cases.10–12 Common atrium (90%), transposition of the great arteries (80%), pulmonary atresia or stenosis (80%), double-outlet right ventricle (80%), and total anomalous pulmonary venous return (70%) are also commonly associated with asplenia (Table 19–1).7,10,12
TABLE 19–1
Incidence of Cardiovascular Abnormalities in Asplenia and Polysplenia Syndromes
| Asplenia | Polysplenia | |
| Atrial septal defect | 90% | 80% |
| Atrioventricular septal defect | 85% | 40% |
| Azygous continuation of the inferior vena cava | Rare | 70% |
| Bilateral superior vena cava | 50% | 40% |
| Dextrocardia | 40% | 40% |
| Double-outlet right ventricle | 80% | 40% |
| Left pulmonary isomerism | Rare | 60% |
| Partial anomalous pulmonary venous connection | Rare | 40% |
| Pulmonary stenosis, pulmonary atresia | 80% | 30% |
| Right pulmonary isomerism | 70% | 10% |
| Single ventricle | 50% | 10% |
| Subaortic stenosis | Rare | 40% |
| Total anomalous pulmonary venous connection | 70% | Rare |
| Transposition of the great arteries | 80% | 30% |
Data from Gutgesell HP: Cardiac malposition and heterotaxy. In: Garson A, Bricker JT, McNamara DG (eds): The Science and Practice of Pediatric Cardiology, vol 2. Philadelphia, Lea & Febiger, 1990, p 1292.
Asplenia was first described by Ivemark in 1955.6,8 From a review of 69 cases, he postulated that because the atrioventricular canal and the conotruncus undergo division simultaneous with the development of the splenic primordia, a single embryological insult could adversely affect both cardiac and splenic development. Asplenia also bears the name Ivemark syndrome.7
In the majority of cases, the stomach, liver, and gallbladder are situs ambiguous; however, situs inversus and solitus are also possible.7 The gallbladder is frequently absent, and dextrocardia or mesocardia is found in 55% of patients.13 Additionally, absence of the intrahepatic inferior vena cava with collateral drainage through the azygous or hemiazygous vein has been reported in 65% to 94% of patients with polysplenia.14–16
Cardiac defects occur in 90% to 95% of cases of polysplenia. Although they are typically less severe than those found in asplenia (see Table 19–1), they are still the leading cause of death associated with this syndrome.17–19
A common atrium occurs in approximately 80% of cases. Left-sided cardiac obstruction appears to occur more frequently in polysplenia than in asplenia. However, other cardiac anomalies that are prevalent in asplenia (such as total anomalous pulmonary venous connection) are rarely associated with polysplenia. Complete heart block has been reported in 50% of fetuses with the polysplenia syndrome.13 Other anomalies include atrioventricular septal defects (60%–70%) and transposition of the great arteries (20%).12
Polysplenia and asplenia are two separate, distinct entities. The majority of cases of left isomerism are discovered during fetal life, whereas right isomerism is typically diagnosed postnatally.7
Embryology
Cardiosplenic syndromes are not a specific disease but a spectrum of abnormalities that involve the abdominal viscera and the cardiovascular system. From an embryological standpoint, polysplenia and asplenia syndromes are thought to be the result of a midline developmental field defect.2,20 Opitz and Gilbert21 defined developmental fields as units of the embryo in which the development of complex structures are determined and controlled in a spatially coordinated, temporally synchronous, and epimorphically hierarchical manner. This means that an insult to this delicate space-time balance may give rise to complex malformations, including errors in symmetry or laterality. An embryogenic insult occurring between the twenty-eighth and thirty-fifth days of gestation has been postulated to result in the spectrum of developmental abnormalities that is considered asplenia or polysplenia.22–24
The specific embryology of many of the associated cardiac abnormalities is discussed in the chapters dealing with each malformation. Generally, it appears that the sequence of cardiac development is arrested in patients with cardiosplenic syndromes during the fifth week of gestation.23–25 In normal development, growth of the endocardial cushions and septation of the conotruncus occur at this time. Additionally, during this embryological period lobation of the lungs and rotation of the gut begin. The connection between the atria and the pulmonary venous plexus is established by 30 to 32 days of gestation.10,22
It should be borne in mind that, although the syndrome of right atrial isomerism is usually associated with asplenia, this is not invariable, and a normal spleen has been reported in some cases.26 Conversely, patients with polysplenia syndrome and left atrial isomerism have been found to have a solitary spleen.
There is clearly considerable overlap in the cardiac abnormalities associated with these two syndromes, but the most specific marker of the polysplenia syndrome appears to be azygos continuation of the inferior vena cava.2,17,19,27–38 This finding has rarely been reported in cases of asplenia.
Abnormalities of systemic and pulmonary venous connections occur in both syndromes. Additionally, hearts with right atrial isomerism exhibit a higher incidence of abnormal ventriculoarterial connections, with double-outlet right ventricle and transposition of the great arteries occurring in more than 75% of cases.26 Conversely, hearts with left atrial isomerism demonstrate a normal ventriculoarterial connection in approximately 70% of reported cases.17
Most cases of polysplenia and asplenia syndromes are sporadic. However, familial occurrence of these syndromes has been described.39–42 The coexistence of asplenia and polysplenia in sibships has also been reported.40,42,43 The occurrence of these sibships, together with the findings of consanguinity in some sporadic cases, suggests autosomal recessive inheritance with reduced penetrance.44–46
Occurrence Rate
The occurrence rate for heterotaxy syndromes is 1 in 10,000 live births or in 0.8% of all patients with congenital heart disease.47,48
A predominance of left isomerism over right isomerism in utero has been well documented.7,16,49 In contrast, postnatally right atrial isomerism appears more common than left atrial isomerism.2,11,50–52
It has been postulated that, although the severity and complexity of congenital heart disease is greater in right atrial isomerism, the increased incidence of complete heart block in conjunction with atrioventricular valve insufficiency associated with left atrial isomerism often leads to congestive heart failure, hydrops fetalis, and death in utero.49
The occurrence rate in siblings of patients with asplenia is reported to be approximately 5%.40,44,52–56 A tendency for asplenia syndrome to occur more frequently in males and for polysplenia syndrome to occur more often in females has been suggested.2,26 Also, right atrial isomerism tends to be more common then left isomerism in the Asian population.7,48
Sonographic Criteria
The most consistent indicators of polysplenia appear to be an interrupted inferior vena cava with a large azygous vein continuation into the superior vena cava and heart block in the presence of structural heart disease. Yildirim et al16 observed these findings in 94% of their cases.
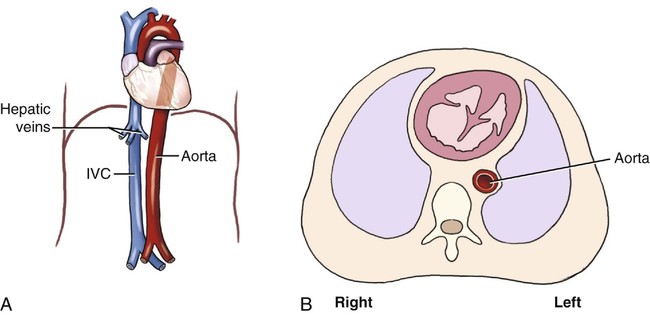
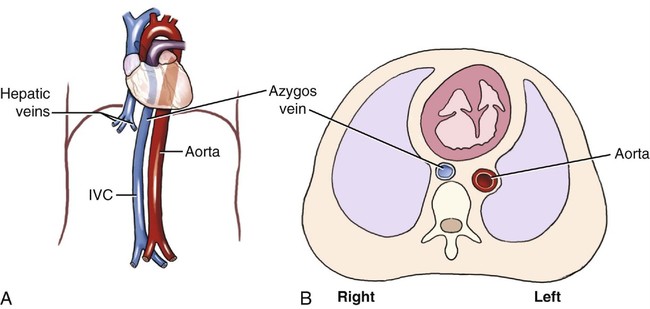
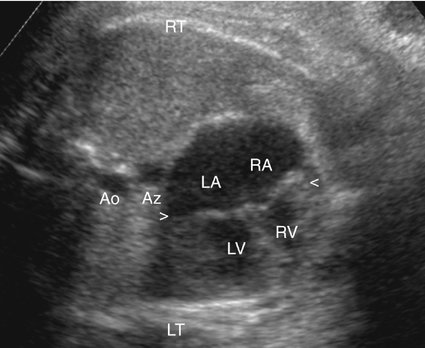
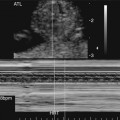
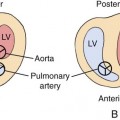
Sheley et al13 reviewed the prenatal sonographic findings in eight fetuses with polysplenia. Interruption of the inferior vena cava with azygous continuation was seen in all eight patients. The authors diagnosed this finding by identifying what they termed the double-vessel sign: two vessels of similar size in a paraspinous location posterior to the heart. Compared with the normal relationship, which shows only the aorta posterior to the heart (Fig. 19–1), interruption of the inferior vena cava results in collateral flow through the azygous vein, which becomes enlarged and readily visible (Fig. 19–2). Therefore two vessels are seen at the level of the heart in a paraspinous location (Fig. 19–3). The azygous veins in their study ranged in diameter from 6 to 12 mm. They did report one false-positive diagnosis of inferior vena cava interruption with azygous continuation in a fetus with asplenia. At autopsy, a large left-sided superior vena cava in this fetus as the likely explanation for the sonographic finding.
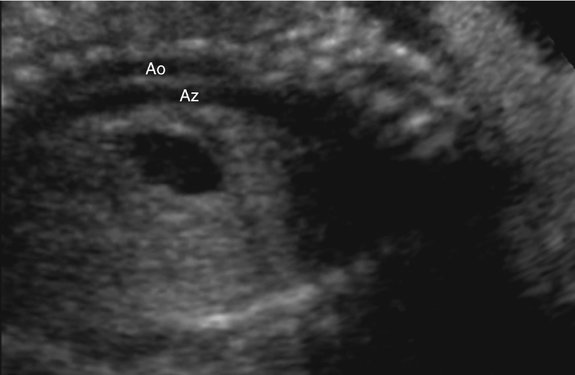
Azygous continuation of an interrupted inferior vena cava may also be visualized in a sagittal view of the fetus. In this projection it will appear as a long vessel running parallel with the aorta, extending to the superior vena cava (Fig. 19–4).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


