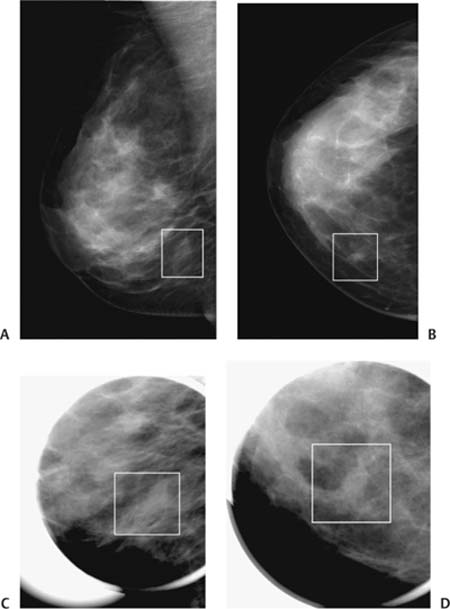
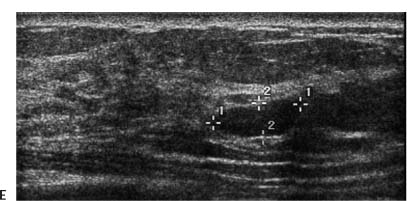
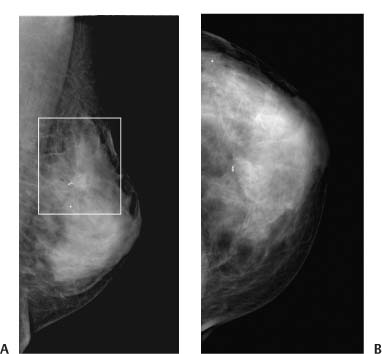
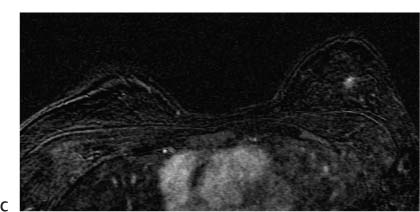
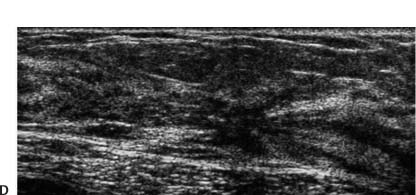
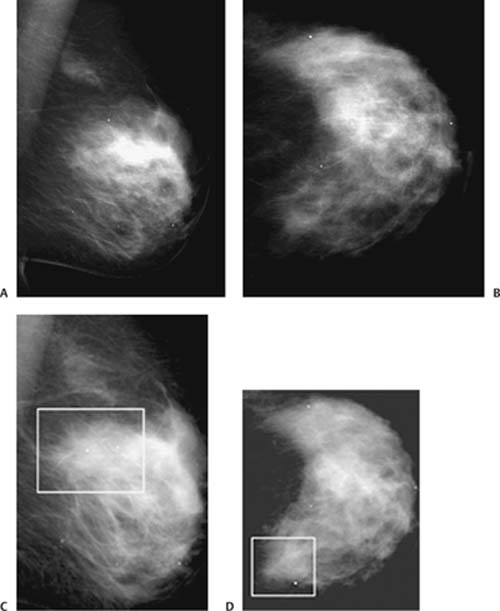
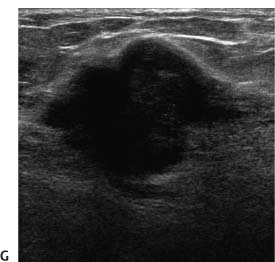
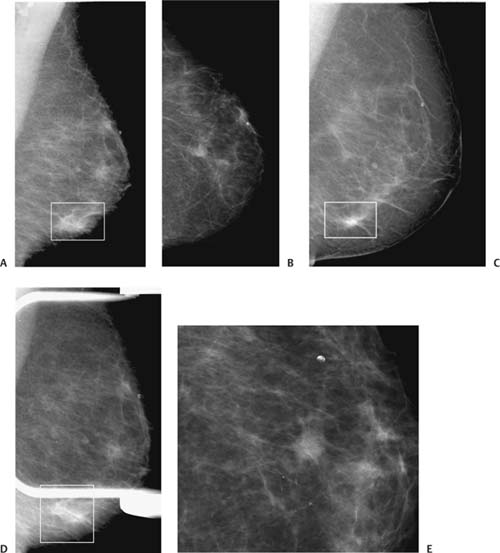
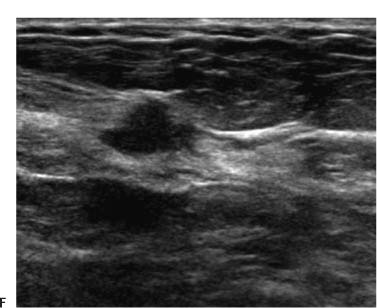
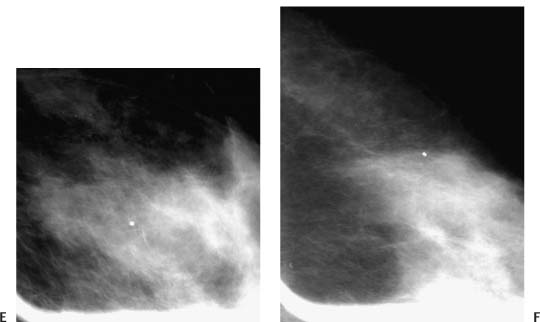
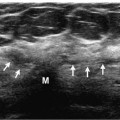
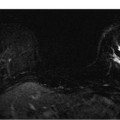
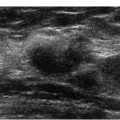
Special Features Asymmetry Clinical History A 38-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 7–3 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) right CC, (C) right MLO spot compression, and (D) right CC spot compression views. There is an ill-defined oval focal asymmetry (square) in the inferior inner breast. Figure 7–3 (E) Right breast sonogram. The mammographic asymmetry corresponds to an oval solid hypoechoic mass. Management BI-RADS category 4, suspicious. Biopsy should be considered. Pathologic Diagnosis Benign Fibroadenoma • On the basis of the sonogram, this mass may be assessed as probably benign (category 3). However, the poorly defined mammographic margins contributed to assessing this lesion as a category 4A. Special Features Asymmetry Clinical History A 48-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 7–4 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Left MLO and (B) left CC mammograms. In the MLO view, there is a focal asymmetry with architectural distortion (square). The biopsy clip marks the location of this lesion in both views. Magnetic Resonance Imaging Figure 7–4 (C) Bilateral breast MRI (subtraction series: 2 minutes after injection of contrast). Initial ultrasound examination is negative, so an MRI is performed. In the left breast, there is a small enhancing lesion in the 12 o’clock position that corresponds to the mammographic asymmetry. Figure 7–4 (D) Left breast sonogram. After magnetic resonance imaging (MRI), the sonographic exam identified a spiculated solid mass that corresponds to both the MRI and the mammogram. Management BI-RADS category 4, suspicious. Biopsy should be considered. Pathologic Diagnosis Benign Radial sclerosing lesion (radial scar) • Radial scars are a diagnostic challenge because they commonly present as architectural distortions with or without focal asymmetry in only one view. The reason these lesions are commonly identified in only one position mammographically is that they are similar to surgical scars in shape: in one plane, they are broad, but in the orthogonal plane, they are extremely thin. This planar shape is also generally evident sonographically. Special Features Asymmetry Clinical History An 82-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 7–5 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Left MLO mammogram. (B) Left CC mammogram 1 year prior. (C) Left MLO mammogram. (D) Left CC mammogram, current exam. Since the previous year (A and B), an asymmetry has developed in the upper inner quadrant. Figure 7–5 (E) Left MLO spot compression mammogram. (F) Left CC spot compression mammogram. Spot compression views did not clarify the margins of this asymmetry. Ultrasonography Figure 7–5 (G) Left breast sonogram. In the 10:30 position, the mammographic asymmetry corresponds to an irregular hypoechoic solid mass. Management BI-RADS category 4, suspicious. Biopsy should be considered. Pathologic Diagnosis Malignant Infiltrating ductal carcinoma • New asymmetries were previously described as neodensities or developing densities: areas in which the tissues are increasingly radiopaque, but the focus or region cannot be characterized as a mass. When the asymmetry is localized in multiple views, sonography is a useful method to further characterize and assess the asymmetry. Special Features Asymmetry Clinical History A 68-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 7–6 Mediolateral (ML), mediolateral oblique (MLO), and craniocaudal (CC) views. (A) Left MLO, (B) left CC, (C) left ML, (D) left MLO spot compression, and (E) left CC spot compression mammograms. In the CC view, there is a central oval asymmetry with spiculations. This asymmetry is not well identified on the MLO view. In retrospect, the lesion is at 6 o’clock (marked by a square on MLO, ML, and MLO spot compression views), so the MLO spot compression views are too high and do not localize the lesion. Figure 7–6 (F) Left breast sonogram. At the 6 o’clock position, there is an irregular hypoechoic solid mass that corresponds to the mammographic asymmetry. Management BI-RADS category 4, suspicious. Biopsy should be considered. Case 7–1
Case 7–1
Pearls and Pitfalls
 Case 7–2
Case 7–2
Pearls and Pitfalls
 Case 7–3
Case 7–3
Pearls and Pitfalls
 Case 7–4
Case 7–4
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


