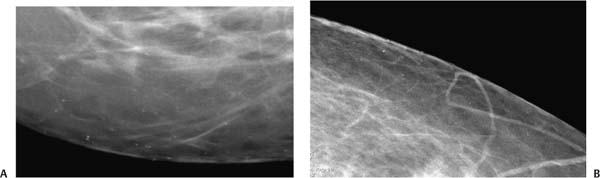
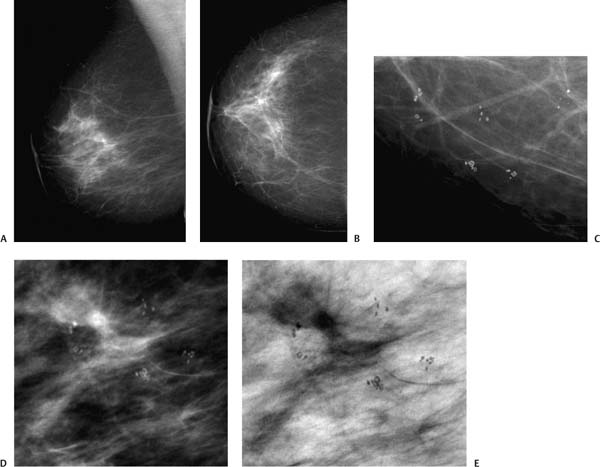
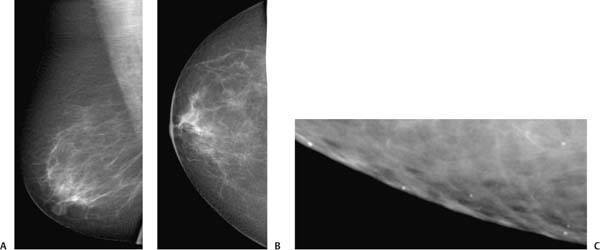
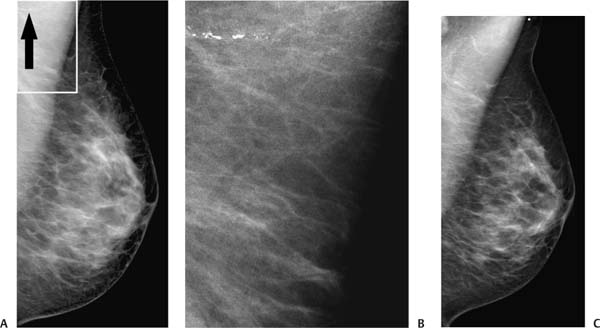
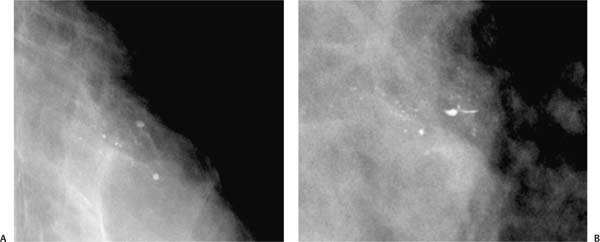
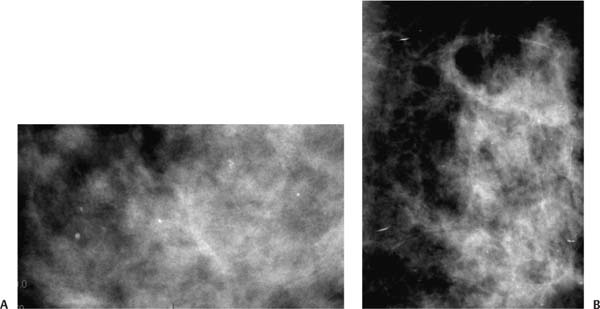
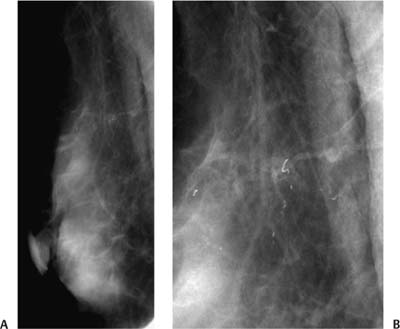
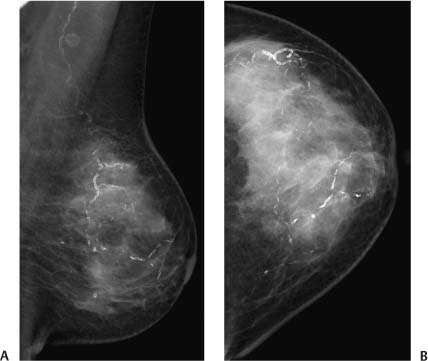
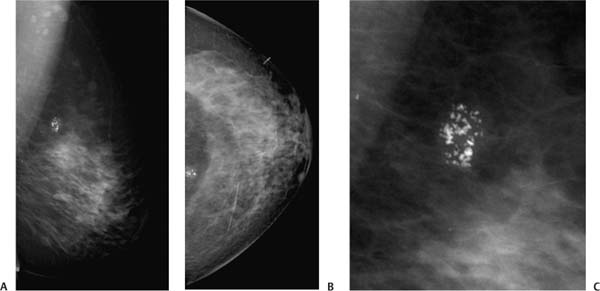
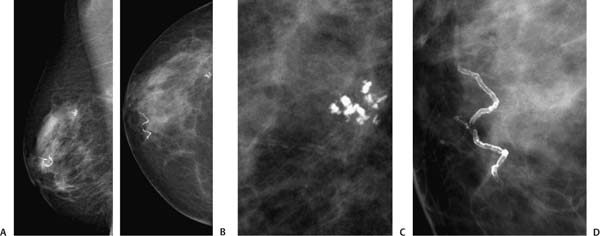
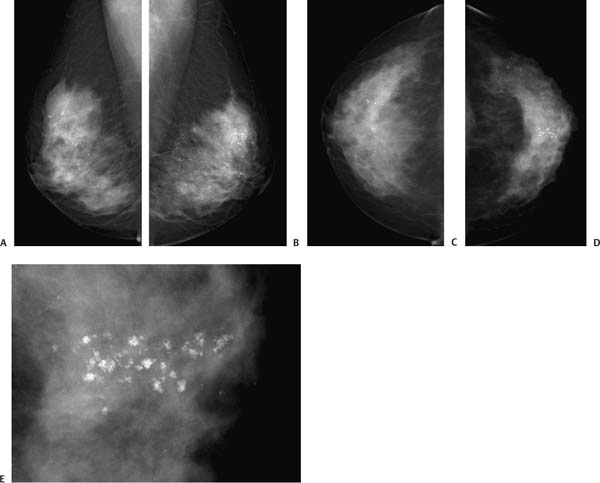
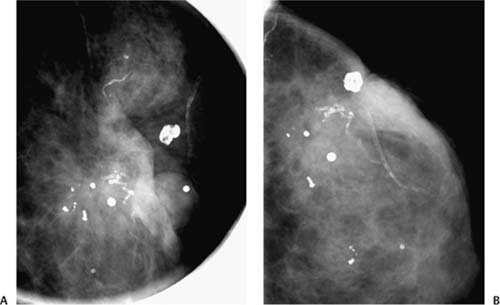
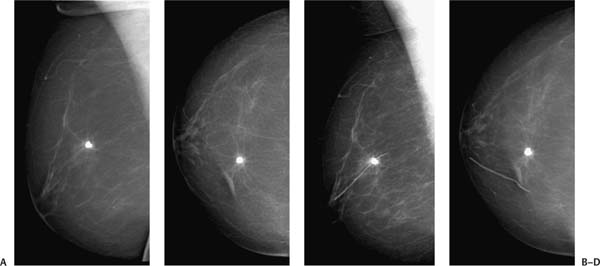
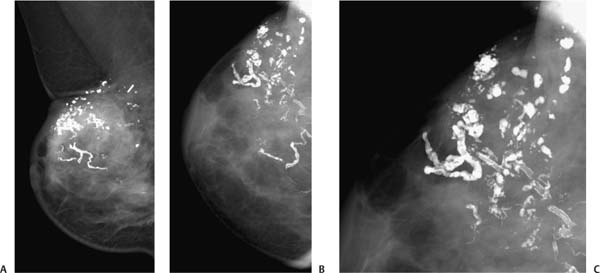
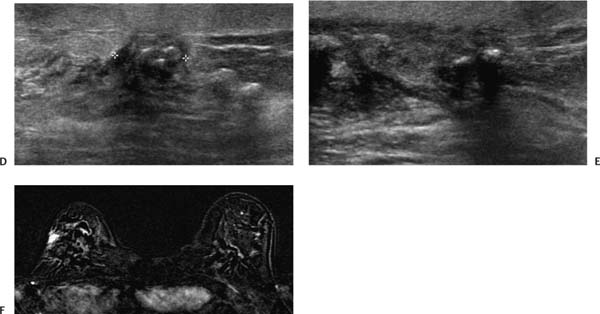
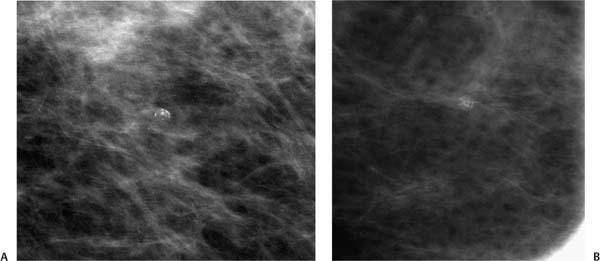
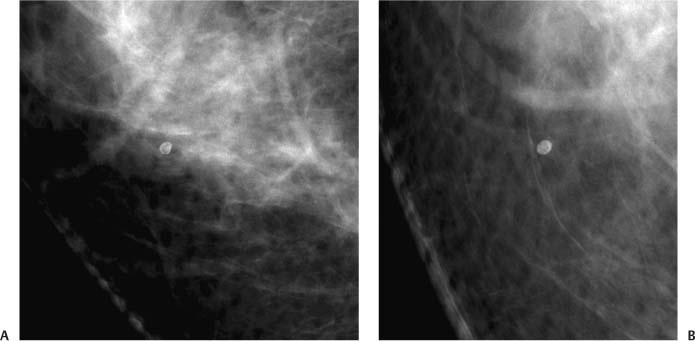
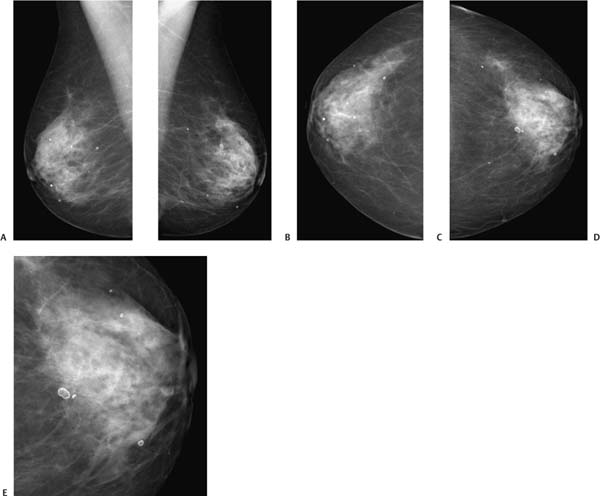
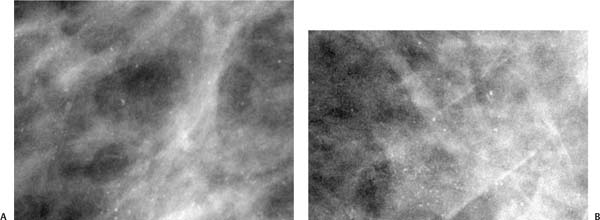
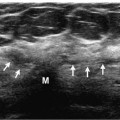
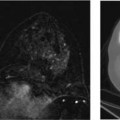
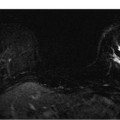
Calcification Morphology Skin calcifications Distribution of Calcifications Diffuse/scattered Clinical History A 64-year-old woman who has had bilateral breast cancers presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–1 Mediolateral (ML) and craniocaudal (CC) views. (A) Left ML magnified tangential and (B) left CC magnified tangential mammograms. There are scattered punctate and round calcifications in the inferior breast. These magnified tangential views demonstrate that the calcifications are within the skin. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Skin calcifications • Digital mammography is particularly better than screen-film mammography in identifying skin calcifications. If it is unclear whether the calcifications are within the skin, an electronic grid can be used to localize the calcifications while the patient is still in compression; a radiopaque marker is then placed on the skin over the position of the calcifications. Using this marker, a tangential magnified image of the skin is taken. Because digital mammography does not require film processing, it is much faster than screen-film mammography. Calcification Morphology Skin calcifications Distribution of Calcifications Diffuse/scattered Clinical History A 56-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–2 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) right CC, (C) right CC magnification, (D) right MLO magnification, and (E) right MLO magnification with white and black inverted. At the 3 o’clock position in the right breast, there are some scattered round and oval calcifications with lucent centers. The magnification CC view (C) demonstrates that the calcifications are within the skin. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Skin calcifications • Besides highly magnifying images, digital mammography can invert the black-and-white presentation, which sometimes clarifies the appearance of calcifications. In this case, the skin calcifications exhibit pathognomonic lucent centers. Calcification Morphology Skin calcifications Clinical History A 59-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–3 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) right CC, and (C) right MLO digitally enlarged. In the right inferior outer breast, there are scattered punctate calcifications. With digital magnification of the screening views (C), it can be seen that these calcifications are within the skin. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Skin calcifications • This case illustrates that digital mammography increases the flexibility of the radiologist to analyze screening mammograms. The skin calcifications could be easily identified on the screening views. Usually, skin calcifications are not identified with screen-film technique because the skin is too dark. • The MLO used for illustrating this case did not demonstrate the nipple in profile. An additional MLO had been performed with acceptable positioning, but this MLO demonstrated the benign calcifications better. Calcification Morphology Miscellaneous Clinical History A 44-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–4 Mediolateral oblique (MLO) views. (A) Left MLO mammogram and (B) enlargement of axillary section of MLO mammogram. There is a thick, coarse linear density in the axilla that is visible only on the MLO view. (C) Left MLO mammogram. After cleaning the axilla, the linear density has disappeared, consistent with skin contamination, such as deodorant. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Deodorant • Antiperspirants commonly contain aluminum, which may produce mammographic densities. Other skin creams containing metallic compounds, such as zinc oxide in sunscreen and tattoos, are also radiopaque. Generally, the large size and axillary location of such lesions suggest a benign etiology, but when faint, they sometimes are confused as suspicious. If there is uncertainty, careful skin cleansing will eliminate or greatly reduce their number. Calcification Morphology Milk of calcium Distribution of Calcifications Diffuse/scattered Clinical History A 52-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–5 Craniocaudal (CC) and mediolateral (ML) views. (A) CC magnification and (B) ML views. In the CC view, the calcifications are round or oval and slightly indistinct. In the ML view, the calcifications form curvilinear densities. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Milk of calcium • Milk of calcium is precipitated calcium within microcysts. With a horizontal beam (ML or lateromedial [LM] views), the calcium layers at the bottom of the cysts and forms curvilinear or linear densities. With a vertical beam (CC view), the calcium forms ill-defined round densities. Calcification Morphology Milk of calcium Distribution of Calcifications Diffuse/scattered Clinical History A 50-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–6 Craniocaudal (CC) and mediolateral (ML) views. (A) Left CC magnification and (B) left ML magnification mammograms. In the inferior half of the breast, there are ill-defined oval and round calcifications on the CC view. However, on the ML view, these round calcifications are replaced by linear or semicircular “teacup” calcifications characteristic of milk of calcium. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Milk of calcium • This example demonstrates that manipulating the image with digital mammography is useful even after additional diagnostic views have been performed. Because these calcifications covered a broader area, the original magnified region was relatively large, and the smaller calcifications were difficult to evaluate even with the magnified views. Therefore, further manual digital magnification of the magnified views was useful in examining the entire area and characterizing the smaller calcifications. Calcification Morphology Vascular Clinical History A 46-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–7 Mediolateral oblique (MLO) views. (A) Left spot MLO magnification and (B) enlargement of mammogram. In the upper outer breast, there are a few long tortuous linear calcifications. These are consistent with vascular calcifications. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Vascular calcifications • Vascular calcifications are generally long (>2 mm) and curvilinear. When they are small, they may be mistaken for DCIS. With suspected small vascular calcifications, a wider soft tissue window can be used to identify the blood vessels. Calcifications within the vessels can be followed using magnification. Calcification Morphology Vascular Clinical History A 75-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–8 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Left MLO and (B) left CC mammograms. Curvilinear vascular calcifications are in the lateral and medial breast. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Atherosclerosis • Arterial calcifications are curvilinear long depositions that are solid or tubular (“train track” calcifications). Occasionally, veins thrombose and form tortuous curvilinear calcifications, which are generally 2 to 3 times the thickness of the arteries. Calcification Morphology Coarse/popcorn Clinical History A 56-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–9 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Left MLO mammogram, (B) left CC mammogram, and (C) enlargement of left MLO mammogram. There is a cluster of large, coarse calcifications at the 12 o’clock position. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Fibroadenoma • Fibroadenomas commonly present with large (>0.5 mm), irregularly shaped “popcorn” calcifications. Usually, these calcifications develop peripherally and extend centrally. Calcification Morphology Dystrophic Clinical History An 84-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–10 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) right CC, (C) right enlarged CC posteriorly, and (D) right enlarged CC near nipple. In the upper outer quadrant, there is a cluster of large, coarse dystrophic calcifications consistent with a fibroadenoma (C). These calcifications have been stable for more than 5 years. Vascular calcifications (D) are in the 3 o’clock position near the nipple. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Fibroadenoma • Fibroadenomas are the most common benign solid mass in women. About 25% of women autopsied have fibroadenomas. After menopause, fibroadenomas commonly involute, forming large, coarse calcifications. Calcification Morphology Dystrophic Clinical History A 65-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–11 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) left MLO, (C) right CC, (D) left CC, and (E) left enlarged CC. There are scattered bilateral large, coarse dystrophic calcifications. These calcifications have been stable for more than 5 years. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Dystrophic calcifications • The large size and scattered distribution are characteristics of benign calcifications. Calcification Morphology Dystrophic Clinical History An 86-year-old woman who had a lumpectomy 14 years ago presents for screening. Physical Examination Negative exam. No change is seen in left breast scar. Radiologic Findings Mammography Figure 5–12 Mediolateral (ML) and craniocaudal (CC) views. (A) Left ML spot magnification and (B) left CC spot magnification views. There are multiple large round, lobular, and irregular calcifications. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Dystrophic calcifications within scar • These large calcifications are characteristic of fat necrosis and dystrophic calcifications within scar. Calcification Morphology Dystrophic Clinical History A 74-year-old woman presents for screening. She had a right lumpectomy for breast cancer 14 years ago. Physical Examination Right breast: Normal exam. Well-healed lumpectomy scar. Left breast: Normal exam. Radiologic Findings Mammography Figure 5–13 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO (without scar marker), (B) right CC (without scar marker), (C) right MLO (with scar marker), and (D) right CC (with scar marker). There is a large single calcification at the 12:30 position. Current digital exam did not have scar marker. The previous digital exam scar markers clearly indicate that the calcification is related to the lumpectomy. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Dystrophic calcification • The scar marker does not help in assessing the large single dystrophic calcification. However, the scar marker does help to clarify the etiology of the mild residual architectural distortion from the previous lumpectomy. Calcification Morphology Dystrophic Distribution of Calcifications Regional Clinical History A 75-year-old woman who had a lumpectomy 9 years ago presents for screening. She notes new thickening at the lumpectomy site. Physical Examination Right breast: In the upper outer quadrant, there is firmness associated with the lumpectomy scar. Left breast: Normal exam. Radiologic Findings Mammography Figure 5–14 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) right CC, and (C) right ML spot magnification mammograms. There are numerous large, coarse, irregular calcifications in the right upper outer quadrant. Curvilinear vascular calcifications are also present. Figure 5–14 (D) Right radial and (E) right aradial sonographic images. Sonographic examination of the lumpectomy site demonstrated a hypoechoic irregular solid mass with architectural distortion, large shadowing calcifications, and skin thickening. These findings are nonspecific for scar or recurrence. (F) Bilateral breast three-dimensional contrast-enhanced dynamic magnetic resonance, subtraction image (2 minutes after contrast injection). Moderate early contrast enhancement of the lumpectomy scar is followed by a plateau in intensity. This kinetics pattern is non-specific, so biopsy was performed. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Scar • The large irregular calcifications are characteristic of dystrophic calcifications associated with scar. • Although the calcifications are benign, the patient’s lumpectomy site was further worked up because of her new clinical symptoms. Calcification Morphology Eggshell/rim Clinical History A 50-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–15 Mediolateral (ML) and craniocaudal (CC) views. (A) Right CC spot magnification mammogram and (B) right ML magnification mammogram. In the right upper inner breast, there is a single round eggshell calcification. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Cyst calcification • Eggshell calcification indicates calcification of a cystic process—usually an oil cyst, rarely a fluid cyst. Digital mammography is much better in characterizing these cysts because a wider gray scale window can be used to demonstrate the nonuniformity of the calcification. Calcification Morphology Round Clinical History A 55-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–16 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO and (B) right CC mammograms. At the 3 o’clock position, there is a single oval calcification. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Fat necrosis • Fat necrosis has many appearances; one of the most common is the oil cyst. The oil cyst is an oval or round calcified circumscribed mass. Calcification Morphology Round Distribution of Calcifications Diffuse/scattered Clinical History A 73-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–17 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) left MLO, (C) right CC, (D) left CC, and (E) left CC enlarged. There are bilateral round and oval well-defined calcifications illustrative of oil cysts. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Fat necrosis • Although oil cysts are a form of fat necrosis, commonly patients with oil cysts have no history of previous injury or surgery. Calcification Morphology Punctate Distribution of Calcifications Diffuse/scattered Clinical History A 57-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 5–18 Mediolateral (ML) and craniocaudal (CC) views. (A) Right ML magnification and (B) right CC magnification mammograms. There are scattered punctate and round calcifications throughout the breast. Management BI-RADS category 2, benign finding Pathologic Diagnosis Benign Sclerosing adenosis • The round shape and scattered distribution are characteristic of sclerosing adenosis. Case 5–1
Case 5–1
Pearls and Pitfalls
 Case 5–2
Case 5–2
Pearls and Pitfalls
 Case 5–3
Case 5–3
Pearls and Pitfalls
 Case 5–4
Case 5–4
Pearls and Pitfalls
 Case 5–5
Case 5–5
Pearls and Pitfalls
 Case 5–6
Case 5–6
Pearls and Pitfalls
 Case 5–7
Case 5–7
Pearls and Pitfalls
 Case 5–8
Case 5–8
Pearls and Pitfalls
 Case 5–9
Case 5–9
Pearls and Pitfalls
 Case 5–10
Case 5–10
Pearls and Pitfalls
 Case 5–11
Case 5–11
Pearls and Pitfalls
 Case 5–12
Case 5–12
Pearls and Pitfalls
 Case 5–13
Case 5–13
Pearls and Pitfalls
 Case 5–14
Case 5–14
Pearls and Pitfalls
 Case 5–15
Case 5–15
Pearls and Pitfalls
 Case 5–16
Case 5–16
Pearls and Pitfalls
 Case 5–17
Case 5–17
Pearls and Pitfalls
 Case 5–18
Case 5–18
Pearls and Pitfalls
 Case 5–19
Case 5–19
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


