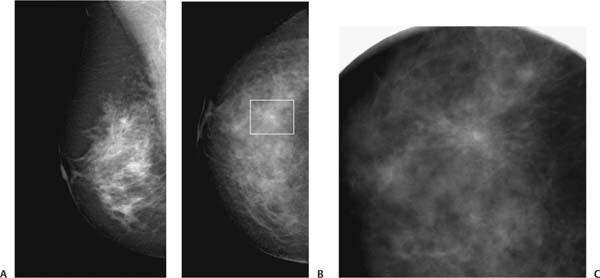
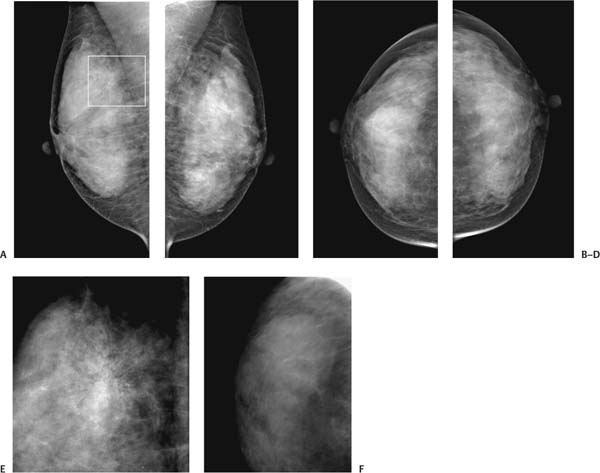
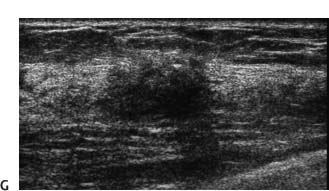
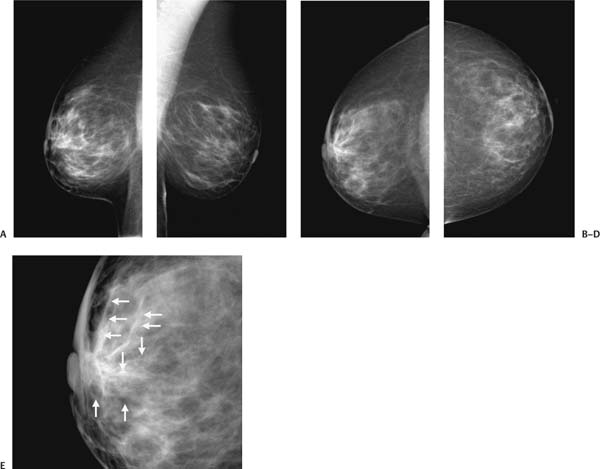
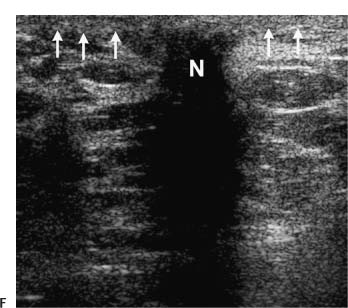
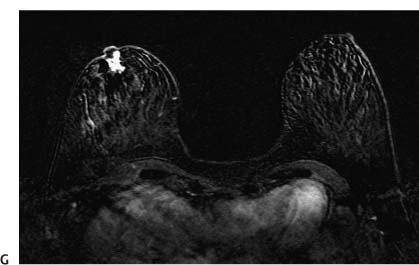
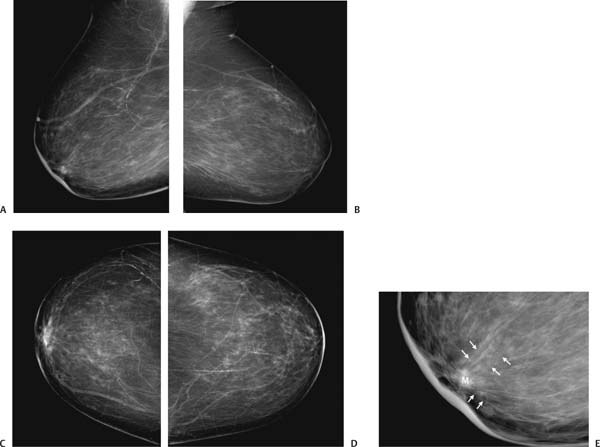
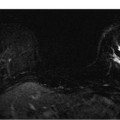
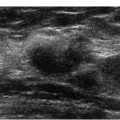
Special Features Architectural distortion Clinical History A 72-year-old woman who had previous benign right breast biopsy presents for screening. Physical Examination Right breast: Faint scar near the 12 o’clock position. Radiologic Findings Mammography Figure 8–1 Mediolateral oblique (MLO) and craniocaudal views. (A) Right MLO, (B) right CC, and (C) right CC spot compression mammograms. In the 12 o’clock position, there is architectural distortion (noted by a square in the CC view) associated with retraction of the posterior edge of the parenchyma. The architectural distortion appears more prominent than in previous exams. Management BI-RADS category 4, suspicious. Biopsy should be considered. Pathologic Diagnosis Benign Scar • Lesions distort the posterior edge of the parenchyma in two ways: either by creating a curvilinear bulge or by retracting the edge. The retraction of the edge creates a V shape, which has been labeled the “tent sign.” Special Features Architectural distortion Clinical History A 41-year-old woman presents for screening. Physical Examination Normal exam Radiologic Findings Mammography Figure 8–2 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) left MLO, (C) right CC, (D) left CC, (E) right MLO spot compression, and (F) right CC spot compression mammograms. In the right 12 o’clock position, there is architectural distortion that is better identified on the MLO views (marked with a square on the MLO view). Figure 8–2 (G) Right breast sonogram. The mammographic architectural distortion corresponds to an irregular, hypoechoic solid mass. Management BI-RADS category 5, highly suggestive of malignancy Pathologic Diagnosis Benign Radial sclerosing lesion (radial scar) • Lesions with architectural distortion are some of the most suspicious abnormalities in the breast. Unless the distortion is due to a benign scar, a spiculated lesion, even when visible in only one view, is highly suspicious when it corresponds to an abnormal sonographic mass. Special Features Architectural distortion Clinical History A 34-year-old woman has difficulty breast-feeding her baby from the right breast. Physical Examination Right breast: Subareolar lump present. Left breast: Normal exam. Radiologic Findings Mammography Figure 8–3 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) left MLO, (C) right CC, and (D) left CC mammograms. (E) Enlargement of C. There is skin thickening and trabecular coarsening (arrows in E) in the right periareolar and subareolar area. Figure 8–3 (F) Right breast sonogram. Under the nipple (N), there is a solid, hypoechoic, heavily shadowing mass. Skin thickening (arrows) is also apparent. Magnetic Resonance Imaging Figure 8–3 (G) Bilateral breast MRI (subtraction series: 2 minutes after injection of contrast). There is an abnormally enhancing right subareolar mass extending into the nipple. Management BI-RADS category 4, suspicious. Biopsy should be considered. Pathologic Diagnosis Malignant Infiltrating ductal carcinoma • About 1 in 3000 to 10,000 pregnancies will be complicated by breast cancer. The most common symptoms are a palpable lump or bloody nipple discharge. Studies have found that more than three quarters of all pregnant patients with breast cancer have mammographic abnormalities. The most common histology of these patients is infiltrating ductal carcinoma. Special Features Architectural distortion Clinical History A 90-year-old woman notes new nipple inversion. Physical Examination Right breast: Nipple inversion associated with subareolar firmness. Left breast: Normal exam. Radiologic Findings Mammography Figure 8–4 Mediolateral oblique (MLO) and craniocaudal (CC) views. (A) Right MLO, (B) left MLO, (C) right CC, and (D) left CC mammograms. (E) Enlargement of (A) There is a right subareolar spiculated mass (M) with periareolar skin thickening and spiculations (arrows). Case 8–1
Case 8–1
Pearls and Pitfalls Pearls and Pitfalls
 Case 8–2
Case 8–2
Pearls and Pitfalls
 Case 8–3
Case 8–3
Pearls and Pitfalls
 Case 8–4
Case 8–4
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


