Key Points
- ▪
Familiarity with the range of vascular complications that may be detected by ultrasound, and their respective findings, is critical.
- ▪
Patients may have more than one complication.
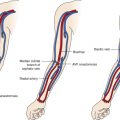
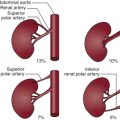
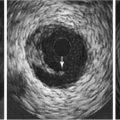
Catheterization-related complications detectable by ultrasound include hematomas ( Figs. 6-1 to 6-3 ), false aneurysms ( Figs. 6-4 to 6-10 ), arteriovenous fistulas ( Figs. 6-11 to 6-17 ), bleeding tracts, thrombosis ( Figs. 6-18 to 6-20 ), dissection, and malpositioned devices ( Figs. 6-21 to 6-23 ). The incidence is variable and depends on the access site attempted/used, the urgency of the procedure, operator experience, degree of patient obesity, size of the catheters, and number of prior catheterizations at that site. Complications that are generally inapparent on duplex examination include embolization of small debris, such as atheroembolism.












Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


