56 Caudal Epidural Block
The sacral hiatus is the caudal termination of the sacral canal. The volume of the epidural space within the sacral canal is highly variable, with estimates ranging from 10 to 26 mL in adults (Table 56-1).1 In this study of 37 adults (23 female, 14 male), the sacrococcygeal membrane was significantly thicker in females than in males (mean values, 3.6 and 2.5 mm, respectively).1 The sacral canal volume was significantly smaller in females than in males (mean values 13.2 and 16.5 mL, respectively).1 Because the sacral canal volume varies, the dose required to achieve a given level of caudal epidural block varies from individual to individual.
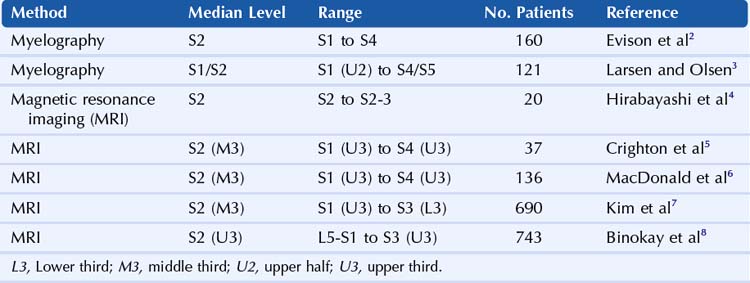
Table 56-1 Magnetic Resonance Imaging Estimates of Caudal Space Anatomy in Adults
| Mean Value | Range | |
|---|---|---|
| PATIENT DATA | ||
| Height (cm) | 168 | 150-183 |
| Weight (kg) | 72 | 49-120 |
| SACROCOCCYGEAL MEMBRANE | ||
| Absence (%) | 10.8 | |
| Thickness (mm) | 3.2 | 1-5 |
| SACRAL CANAL | ||
| Maximum anteroposterior diameter (mm) | 4.6 | 1-8 |
| Angle (degrees) | 57.9 | 40-74 |
| Volume (mL) | 14.4 | 9.5-26.6 |
| DURAL SAC | ||
| Shortest distance from sacrococcygeal membrane to dural sac (mm) | 60.5 | 34-80 |
Adapted from Crighton IM, Barry BP, Hobbs GJ. A study of the anatomy of the caudal space using magnetic resonance imaging. Br J Anaesth 1997;78:391–5.
In adults, the dural sac of the subarachnoid space ends between the S1 and S2 sacral segments.1 In this study, the distance between the dural sac and sacrococcygeal ligament ranged from 34 to 80 mm. The S5 and coccygeal nerves normally exit the sacral canal through the sacral hiatus. The sacral and coccygeal cornua (horns) articulate to form an archlike structure. Table 56-2 summarizes the estimates of the level of the caudal termination of the dural sac in adults gathered from several studies.
Variations in sacral anatomy are relatively common. A number of conditions can make caudal block difficult, including narrowing or complete absence of the sacral hiatus.9,10 These conditions occur in 3% to 6% of anatomic specimens. The sacral cornua are prominent (>3 mm of bony prominence on each side) in only 21% of adult sacrums,9 and therefore assessment by palpation is problematic.
The sacral epidural space is highly vascular. Inadvertent intravenous injection is relatively common during caudal block, occurring in about 5% to 10% of these procedures.11
Landmarks for caudal block are traditionally assessed by palpation. The posterosuperior iliac spines (the superolateral sacral crests of the sacrum) form an equilateral triangle with the sacral hiatus.10 Although this approximation is accurate, the clinical assessment of landmark position can be difficult. Traditional techniques also rely on tactile sense of needle entry into the caudal space. However, the sacrococcygeal ligament is soft in children and may therefore not be easy to detect manually by needle advancement.12
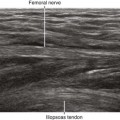
Ultrasound can be used to guide caudal blocks in pediatric and adult patients.13,14 Sonography can determine the location and size of the sacral hiatus for needle tip placement. In addition, ultrasound can be used to image the distribution after caudal epidural injection. However, the bone of the sacrum prevents ultrasound imaging of most of the sacral canal. One concern is that acoustic shadowing from the overlying bone can prevent detection of intravascular injection during caudal blocks, particularly in adults. Ultrasound imaging may be of particular utility in guiding caudal injections in patients with spinal dysraphism.15
Suggested Technique
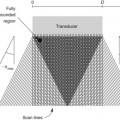
Caudal block with ultrasound is optimally performed in prone position with sterile transducer cover and skin preparation. The wide variety of transducer selections for caudal block depend on patient size.11 In thin adult patients, a 5- to 10-MHz small-footprint “hockey-stick” transducer is appropriate. Average-sized adults image well with a standard linear transducer for the procedure. For obese patients, a lower frequency curvilinear array is optimum.
The sacral hiatus is easiest to image in transverse view over the midline.14 The sacral cornua appear as two reverse U-shaped hyperechoic structures. The sacrococcygeal ligament and base of the sacrum appear as two parallel bandlike structures between the cornua. The sacral hiatus lies between these two hyperechoic bands.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


