Cerebrovascular Anatomy and Regional Blood Supply
Robert Vollmann
Josef Simbrunner
Michael Augustin
Internal Carotid Artery
Basic Anatomic Relationship
The common carotid artery divides into the internal carotid artery (ICA) and external carotid artery (ECA) at the level of the thyroid cartilage (Fig. 40.1). In younger patients, there is a sharp angle and both vessels lie very close to each other. In older patients, where elasticity has decreased, these two vessels depart and the angle at the division becomes more obtuse.1 The ICA runs first lateral toward the ECA and moves in the course toward the cranium medially and dorsally.1
Through the carotid canal, the ICA enters the cranium and divides into its main branches (Fig. 40.2). The ICA supplies blood to the cerebral hemispheres, ipsilateral eye, and parts of the forehead and nose. According to Bouthillier (1996)2 the ICA can be divided into seven segments: cervical (C1), petrosal (C2), lacerum (C3), cavernous (C4), clinoid (C5), ophthalmic (C6), and communicating (C7) segments. Normally, there are no branches from the cervical or petrosal segment.3
 FIGURE 40.1. General anatomy of the carotid and vertebral artery. (Source: Shock First. Anatomical Chart Company, General Anatomy, 2008-05-14 0614, 2008-07-13 1449, with permission.) |
The C1 or cervical portion extends from its junction with the common carotid artery to the external orifice of the carotid canal; the C2 or petrous portion courses within the carotid canal and ends where the artery enters the cavernous sinus; C3 is a small segment that extends from the petrous apex above the foramen lacerum, curving upward toward the cavernous sinus. The C4 or cavernous portion can further be divided into five subsegments (a) the posterior vertical segment, (b) posterior medial genu, (c) horizontal segment, (d) anterior genu, and (e) vertical segment. C4 runs through the cavernous sinus and anastomoses with branches from the external carotid artery through the foramen rotundum, foramen ovale, and foramen spinosum. The C5 segment runs between the
proximal and distal rings of cavernous sinus. It ends as ICA enters the subarachnoid space near the anterior clinoid processus. C6 extends from the distal dural ring at the superior clinoid to just below posterior communicating artery origin. It gives rise to the ophthalmic artery and the superior hypophyseal artery. C7 extends below the posterior communicating artery to the terminal ICA bifurcation where the anterior cerebral artery (ACA) and middle cerebral artery (MCA) arise and passes between optic and oculomotoric nerves.
proximal and distal rings of cavernous sinus. It ends as ICA enters the subarachnoid space near the anterior clinoid processus. C6 extends from the distal dural ring at the superior clinoid to just below posterior communicating artery origin. It gives rise to the ophthalmic artery and the superior hypophyseal artery. C7 extends below the posterior communicating artery to the terminal ICA bifurcation where the anterior cerebral artery (ACA) and middle cerebral artery (MCA) arise and passes between optic and oculomotoric nerves.
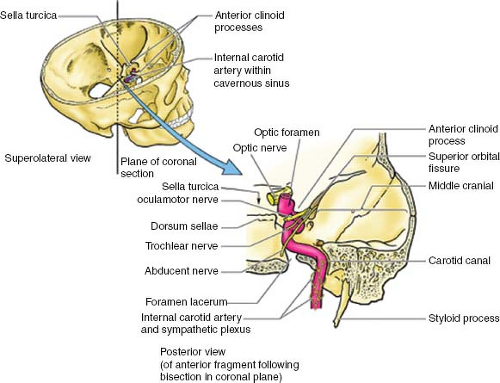 FIGURE 40.2. Cranial pathway of the ICA. (Source: Moore KL, Dalley AF II, Clinical Oriented Anatomy (4th ed.). Baltimore: Lippincott Williams & Wilkins; 1999, with permission.) |
Extradural and Dural Branches
Within the carotid canal, the internal carotid gives off fine caroticotympanic branches. Another fine branch called the ramus canalis pterygoidei penetrates the pterygoid canal.
Two main stems arise from the cavernous portion of the siphon:4
Dorsal stem: basal tentorial branch, clival branch, which anastomoses with the other side, branching to the internal auditory canal.
Lateral stem: marginal tentorial branch, branching to the trigeminal ganglion and branching to cranial nerve IV and V, branches to the wall of the cavernous sinus, meningeal branch to the dura of the middle fossa, which anastomoses with the middle meningeal artery, and orbital branch, which anastomoses with branches of the ophthalmic artery.3
 FIGURE 40.3. Internal carotid artery, lateral view. Anterior choroidal artery (large arrowhead) originating a temporal branch (small arrowheads). Pontochoroidal artery (arrow). (Source: Uflacker R, Atlas of Vascular Anatomy: An Angiographic Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins; p. 2019, with permission.) |
Intradural Branches
Ophthalmic Artery
Anterior Choroid Artery
About 99% of cases the anterior choroid artery originates from the posterior wall of the ICA between the posterior communicating artery and the carotid bifurcation (Fig. 40.4). The anterior choroid artery passes backward to the inferior-medial surface of the optic tract and under it laterally. In most cases, this artery runs along the lateral aspect of the optic tract to the geniculate body. The first portion of this vessel lies within the crural cistern near the middle and posterior aspect of the uncus. It curves laterally near the geniculate body and passes through the wings of the ambient cistern.3
Anterior Cerebral Artery
A systematic description of the ACA has been given by Fisher et al.6 They divided the ACA into precommunicating (A1), anterior communicating artery for the communicating system, A2 below the genu of the corpus callosum, A3 around the genu, and A4 and A5 as the terminal portions (Fig. 40.5).6
Embryologically, a group of lateral striate arteries develop from the proximal ACA stem. For example, the recurrent artery of Heubner develops from this system, as does the MCA and some smaller vessels, which penetrate the hemisphere at the anterior perforated substance.3
 FIGURE 40.4. Dural and extradural branches of the internal carotid artery and external carotid artery. (Source: Uflacker R, Atlas of Vascular Anatomy: An Angiographic Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins; p. 2023, with permission.) |
Two major groups of branches can be detected from the proximal aspect of ACA [2]:
The hypothalamo-chiasmatic branches, which relate to the ventral part of the diencephalic supply. The latter belongs
to the initial portion of the ACA as well as its involvement in the supply of the ophthalmic tract (Fig. 40.6).
The striato-cortical branches include the arteries involved in the supply to the telencephalon and striatum. They also constitute part of the circle of Willis and belong to the diencephalon.
The chiasmatic arteries are anastomosed with the supracavernous ICA branches and pituitary stalk branches.
 FIGURE 40.5. Branches of the anterior cerebral artery. (Source: Alternative Medicine, Anesthesiology/Pain, Chiropractic, General Anatomy, Neurology/Neurosciences, Orthopaedics/Rehabilitation, Physical Therapy, Psychiatry/Psychology & Psychopharmacology, Sports Medicine, 2008-05-14 0721, 2008-07-13 1449, with permission.) |
The recurrent artery of Heubner is one of the vessels of the striato-cortical arterial group. Its territory indicates a consistent supply to the cortex and a termination beyond the anterior perforated substance (Fig. 40.6). It is classically described as an ending in one or two branches, entering the anterior perforated substance.
Middle Cerebral Artery
The MCA originates at the bifurcation of the ICA as the larger and more direct branch than the ACA. It originates lateral to the optic chiasm and courses laterally and slightly anteriorly, inferior to the anterior perforated substance to reach the medial end of the Sylvian fissure (M1). The M1 segment is the sphenoidal segment and lies posterior and parallel to the sphenoidal ridge. The artery then crosses over the limen insulae and enters the insular area, where it divides into its secondary trunks (i.e., the superior and inferior trunks [M2]), referred to as the insular segment. These secondary trunks course over the insular cortex and give rise to the cortical branches. These branches turn around the operculum (M3) and then spread out over the cerebral convexity (M4). M3 is often referred to as the opercular segment and M4 as the cortical segment (Fig. 40.7).
Main Trunk
The MCA outer diameter just proximal to its bifurcation ranges normally from 4 to 5.5 mm. The branches of the main trunk (M1) can be divided into two groups of vessels:
Superolateral group: These branches arise from the superolateral surface of the M1 segment and consist of the uncal artery, polar temporal artery, and the anterior temporal artery. Both the polar temporal artery and anterior temporal artery arise as a common trunk. The polar temporal artery supplies the anterior temporal pole of the superior, middle, and inferior temporal gyri.
Bifurcation
The bifurcation of the MCA occurs at the high point of the limen insulae. The MCA usually divides into the superior and inferior trunks. The area of the bifurcation may also
be described as forming an omega pattern because of the initial divergent and then convergent courses of the secondary trunks (Fig. 40.8).3,4
be described as forming an omega pattern because of the initial divergent and then convergent courses of the secondary trunks (Fig. 40.8).3,4
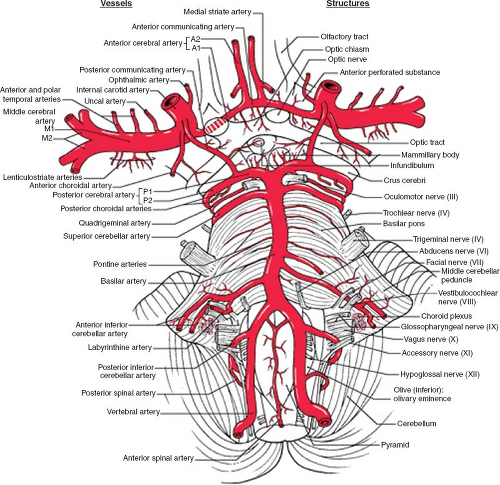 FIGURE 40.6. Perforators and vertebrobasilar system overview. (Source: From Haines DE, Neuroanatomy: An Atlas of Structures, Sections, and Systems, 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2004, with permission.) |
Cortical Branches (M3 and M4)
The cortical branches that are present fairly consistently are the orbito-frontal, prefrontal, precentral, central, posterior parietal, middle temporal, posterior temporal, temporo-occipital, and angular arteries (Fig. 40.9).
Perforating Branches
Based on their morphologic and topographic features, the perforating arteries can be divided into medial, middle, and lateral groups.7
Medial Perforating Arteries
The medial perforating arteries arise from the MCA just distal to the carotid bifurcation and the site of the anterior choroidal artery. They range in number from one to five,
but most often two arteries were present. In almost all cases, the medial vessels branch directly off of the MCA trunk. The medial branches most commonly originate as single vessels.4
but most often two arteries were present. In almost all cases, the medial vessels branch directly off of the MCA trunk. The medial branches most commonly originate as single vessels.4
 FIGURE 40.7. Branches of the middle cerebral artery. (Source: From Haines DE, Neuroanatomy: An Atlas of Structures, Sections, and Systems, 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2004, with permission.) |
 FIGURE 40.8. Frontal view of injection in the right internal carotid artery, showing the lenticulostriate branches and the bifurcation of the middle cerebral artery. (Source: Uflacker R, Atlas of Vascular Anatomy: An Angiographic Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins;, with permission.) |
 FIGURE 40.9. Left internal carotid artery. Anterior choroidal artery (small arrow) with the plexal branches (arrowheads). Posterior division of the middle cerebral artery with a single trunk (large, wide arrow) up to the outlet of the fissure, where it gives origin to the temporo-occipital (1), angular (2), superior parietal (4), and inferior (3) arteries. The postcentral artery (5) originates from the parietal trunk (3, 4), whereas the central (6) originates from the division of the middle cerebral artery (white arrow). Precentral (7) and prefrontal (8) arteries. Orbitofrontal artery (9). (Source: Uflacker R, Atlas of Vascular Anatomy: An Angiographic Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins, with permission.) |
Medial perforating arteries usually course dorsally, caudally, and laterally. Sometimes, however, they run medially at first, forming curves or even loops above the carotid bifurcation, and only later take their final direction.4
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


