Overview
Location
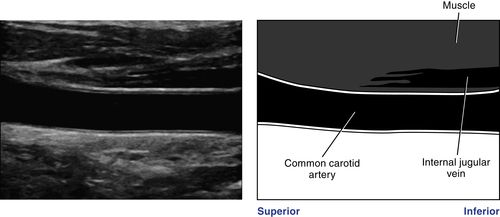
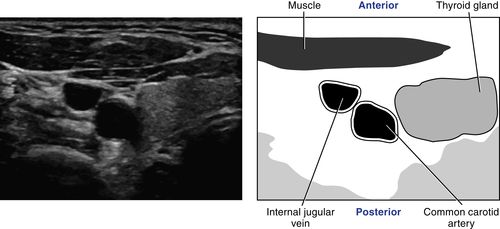
• Medial to internal jugular vein.
• Lateral to thyroid gland.
• Posteromedial to sternocleidomastoid muscle.
Anatomy
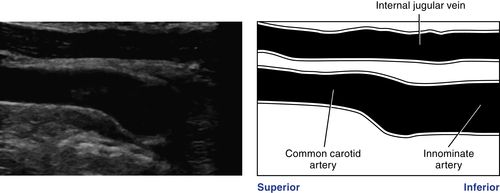
• Right common carotid artery originates from the innominate (brachiocephalic) artery.
• Left common carotid artery originates from the aortic arch.
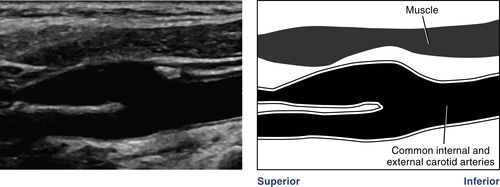
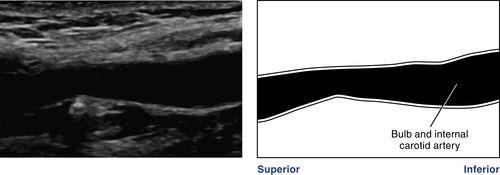
• At the superior border of the thyroid cartilage (vertebrae C2 to C3), the common carotid artery bifurcates into an anteromedial external carotid artery and a posterolateral internal carotid artery. The level and anatomic configuration of the bifurcation are variable. The carotid bulb, which may be referred to simply as the bifurcation, may not be geometrically distinct. The bulb may be part of the common carotid artery and the internal and/or external carotid artery. The external carotid artery may lie posterior and lateral or posterior and medial to the internal carotid artery.
• The external carotid can be differentiated from the internal carotid artery by the presence of branches within the neck. The internal carotid artery normally has no extracranial branches.
• The internal carotid artery usually has a larger diameter than the external, although this is variable.
• The common, internal, and external carotid arteries form the anterior cerebral circulation.
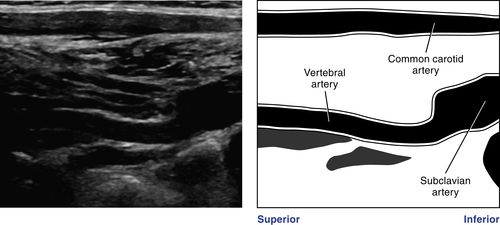
• The vertebral artery originates from the subclavian artery and courses superiorly and posteriorly, entering the transverse processes of the vertebrae at C6 and exiting between C1-C2. The left vertebral artery is often greater in diameter than the right.
• The vertebral arteries join to form the basilar artery. Together, these vessels make up the posterior cerebral circulation.
Physiology
• The common carotid artery provides blood flow to both low- and high-resistance vascular beds. Approximately 80% of the blood flow from the common carotid artery enters the internal carotid artery to supply blood flow to the low-resistance vascular tissues of the brain and eye. Because of this high-flow demand, the Doppler spectral waveform from the common carotid artery is characterized by a low-resistance blood flow pattern. The remaining 20% of the blood flow volume from the common carotid enters the external carotid artery to supply the high-resistance muscular tissues of the face and scalp.
• The internal carotid artery provides blood flow to the low-resistance anterior cerebral circulation. The blood flow pattern of the internal carotid artery is characterized by constant forward diastolic flow.
• The external carotid artery provides blood flow to the high-resistance vascular bed of the muscles of the face, forehead, and scalp. The blood flow pattern of the external carotid artery is characterized by low diastolic flow.
Sonographic Appearance
• In the normal vessel, lumen should be echo-free.
• If viewing the vessel at a perpendicular angle, note that the arterial walls are echogenic. This reflectivity results from acoustic properties of collagen fibers found within the intima and media of the arterial wall and helps to sonographically differentiate arteries and veins.
• Using multiple scan planes, you should be able to image the common carotid artery, the carotid bulb (bifurcation), and the external and internal carotid and vertebral arteries as separate arterial segments.
Preparation
Patient Prep
• None.
Pulsed Doppler Transducers
• 10.0-MHz to 12.0-MHz linear array: offers better resolution, but may not be able to visualize all anatomy if vessels lie deep within the neck.
• 7.5-MHz linear array: allows slightly better penetration.
• 5.0-MHz linear array: may require use of a standoff pad because of decreased resolution unless using a broadband transducer with auto focusing.
• 2.0-MHz to 4.0-MHz curved array: useful for imaging the innominate and proximal left common carotid artery in some patients.
Patient Position
• Supine with the head resting flat or slightly elevated on a thin pillow, and turned slightly away from the side to be scanned. Hyperextension of the neck must be avoided because this will make it difficult to maintain full transducer contact with the skin and may cause the vessels to lie in an inappropriate anatomic plane.
• As the examiner, you should sit at the head of the examination table with the patient’s head directly in front of you. You should be able to rest your elbow on the corner of the table or the end of the pillow. This arm position ensures minimal compression of the carotid vessels by the transducer and an appropriate ergonomic position of your arm and shoulder. You must then scan ambidextrously to be able to reach the ultrasound system easily.
• Alternatively, you may stand beside the examination table and lean one arm across the patient’s chest to reach the neck. Care must be taken to ensure that your arm is supported and not at a right angle to your body. A pillow may be placed over the patient’s chest to ensure his or her comfort.
• The examination may also be performed with the patient in an erect position if he or she is unable to lie down. Care must be taken to ensure that your arm is supported and not at a right angle to your body.
Cerebrovascular Duplex Survey
1. The purpose of the survey is to identify arterial wall abnormalities, vessel tortuosity, pathology, and anatomic anomalies. The initial survey is performed with gray-scale (B-Mode) imaging to ensure that features of the arterial wall and plaque morphology are accurately characterized.
2. Initiate the survey on the right side of the neck immediately superior to the clavicle with the transducer in a transverse scanning plane anterior to the sternocleidomastoid muscle. Identify the jugular vein. Move medially to detect the proximal common carotid artery and identify the thyroid gland.
3. Return to the transverse view of the proximal common carotid artery. Begin the axial survey of the right common carotid artery.
4. Angle as inferiorly as possible to image the origin of the right common carotid artery.
5. Slowly scan superiorly, noting vessel walls, tortuosity, and anatomic anomalies.
6. At the level of the bifurcation make special note of the carotid bulb, the presence of plaque, and the origin of the bifurcation vessels.
7. Continue to follow the course of the internal and external carotid arteries, imaging as far superiorly as possible.
8. Return to the proximal common carotid artery immediately superior to the clavicle.
9. Rotate the transducer 90 degrees to achieve a sagittal scanning plane. Place the transducer anterior to the sternocleidomastoid muscle (or posterior to the muscle in a sagittal scanning plane or laterally in a coronal imaging plane).
10. Move laterally and identify the jugular vein. Move medially through the common carotid artery and identify the thyroid gland.
11. Return to the longitudinal view of the common carotid artery and angle as inferiorly as possible to view the common carotid artery origin, the distal segment of the innominate artery, and the proximal subclavian artery.
12. Return to the longitudinal view of the common carotid artery. Slowly move the transducer superiorly, continuously rocking through the vessel medial to lateral to view as much of the vessel wall as possible.
13. While at the level of the midsegment of the common carotid artery, angle the probe in a posterolateral manner and look for the acoustic shadowing indicating the vertebral bodies. Coursing between the vertebral bodies, you should see the vertebral artery, which commonly lies posterior to the vertebral vein. Angle the probe in a very slight medial/lateral manner to ensure the best visualization of the artery. Follow the course of the vertebral artery inferiorly to its origin from the subclavian artery.
14. Angle the probe anteromedially to return to the common carotid artery survey.
15. Continue to scan superiorly to the level of the bifurcation. Keeping the distal segment of the common carotid artery in view, rock the transducer in an anteromedial/posterolateral motion, and identify the internal and external carotid arteries. Make note of the presence and location of plaque and anatomic abnormalities.
16. Continue to move the transducer superiorly with a slight posteromedial angle to view the internal carotid artery. Continue to rock the transducer lateral to medial to view the length of the vessel walls completely. Follow the vessel walls as far superiorly as possible.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


