Chapter 28 Cervical Transforaminal Epidural Steroid Injection
Cervical transforaminal epidural steroid injections are indicated to relieve radicular symptoms with or without axial neck pain from cervical nerve root irritation. The traditional approach to the epidural space was interlaminar. The transforaminal epidural steroid injection is used to deliver the injectate to the ventral epidural space where the pain generators are located: the posterior annulus, the ventral aspect of the nerve root sleeve, and the neural foramen.1,2
Neurovascular risks for this procedure are high, with known complications thought to be caused by the intravascular injection of particulate steroid, thereby resulting in the embolism of vascular structures with infarction.3–6 Digital subtraction is strongly advised to increase sensitivity to the detection of vascular contrast flow. Note that the trajectory (oblique) view is also one of the multiplanar views. This procedure may be performed in the supine position as demonstrated in this chapter or in the lateral decubitus position.
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
 Trajectory View (
Trajectory View (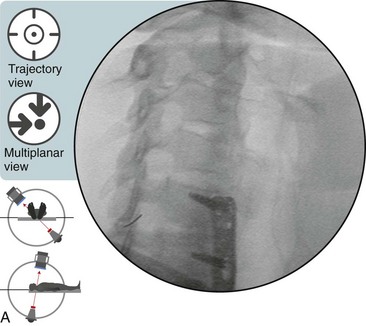
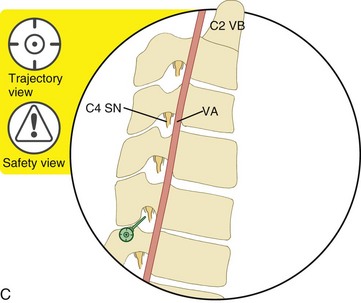
 Safety Considerations
Safety Considerations The Trajectory View (Foraminal Oblique) Is Also a Multiplanar View
The Trajectory View (Foraminal Oblique) Is Also a Multiplanar View
 The patient is positioned supine. Confirm the level with a posteroanterior view by counting down from the C2-3 intervertebral foramen.
The patient is positioned supine. Confirm the level with a posteroanterior view by counting down from the C2-3 intervertebral foramen.

 Tilt the C-arm image intensifier to square off the superior endplate of the vertebral body.
Tilt the C-arm image intensifier to square off the superior endplate of the vertebral body.
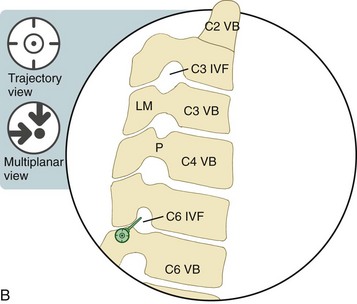
 Adjust the obliquity and the tilt to optimally enlarge the size of the intervertebral foramen.
Adjust the obliquity and the tilt to optimally enlarge the size of the intervertebral foramen.


 Optimal Views in Multiplanar Imaging
Optimal Views in Multiplanar Imaging
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


