Chapter 4 Renal
Adrian Dawkins
4 Questions and Answers
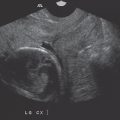
Question 4.1: Longitudinal sonogram of the right kidney obtained in a 35-year-old male with acute renal failure. What anatomic structure is indicated by the arrow ?

Renal cortex.
Renal medulla.
Position of arcuate arteries.
Renal sinus.
Answer:
D. Correct. The area indicated is the echogenic renal sinus fat that surrounds the renal collecting system and vessels.
A. Incorrect. The renal cortex is the outermost layer of the kidney.
B. Incorrect. The medullary pyramids are found deep to the outer renal cortex and form part of the renal parenchyma. They are typically hypo- to isoechoic with respect to the outer cortex.
C. Incorrect. The arcuate arteries are positioned more peripherally within the renal parenchyma and run along the border of the cortex and medullary pyramids.
Question 4.2: Which statement is correct?
In the adult population, the kidneys are usually more echogenic than the normal liver.
When the liver extends below the inferior pole of the right kidney, hepatomegaly is present.
The kidneys move inferiorly with inspiration.
In neonates, the renal cortex is typically hypoechoic with respect to the liver.
Answer:
C. Correct. Both kidneys move inferiorly during inspiration. This maneuver may be used to improve visualization of the kidneys as well as to facilitate image-guided renal biopsies.
A. Incorrect. In the adult patient, the normal kidney is usually hypoechoic with respect to the liver. The renal cortex in this case demonstrates abnormally increased echogenicity secondary to acute tubular necrosis.
B. Incorrect. While the liver may extend below the right kidney in hepatomegaly, this may also be a normal variant, Riedel’s lobe. Other coexisting findings such as rounding of the inferior liver edge or actual volume measurements using 3D ultrasound are better predictors of hepatomegaly.
D. Incorrect. In neonates, the renal cortex is typically hyperechoic with respect to the liver.
Question 4.3: A longitudinal sonographic view of the left kidney is obtained in a 45-year-old male with suspected left renal colic. Which statement is correct?

Ultrasound is the first test of choice in the diagnosis of this condition, in this patient population.
The composition of the calculus may be inferred from the imaging appearances.
Calcium oxalate calculi are the most common type.
Pure uric acid stones are not visible on ultrasound.
Answer:
C. Correct. Renal calculi develop from a variety of reasons and therefore tend to vary in chemical composition. However, roughly 80% of renal calculi are calcium based with calcium oxalate stone accounting for roughly 60% of all calculi.
A. Incorrect. Noncontrast computed tomography (CT) is the investigation of choice in adults and nonpregnant females in the setting of suspected renal colic.
B. Incorrect. The composition of renal calculi cannot be directly inferred from ultrasound appearances alone since stones of differing composition may have similar sonographic appearances.
D. Incorrect. Uric acid stones may not be visible on plain radiographs. However, these stones are dense enough to be discerned sonographically.
Question 4.4: Which statement is correct regarding the stone size?
Spatial compounding is more accurate than harmonic imaging at estimating stone size.
Posterior acoustic shadow width is touted as being a more accurate estimate of true stone size with increasing kidney depth.
The smaller the stone, the more accurate the sonographic measurement.
Ultrasound tends to underestimate the size of stones.
Answer:
B. Correct. With increasing depth, ultrasound tends to overestimate the size of calculi, since the ultrasound beam diverges beyond the focal zone. However, the posterior acoustic shadow cast by the stone is less affected by this phenomenon.
A. Incorrect. Spatial compounding seeks to improve image uniformity by obtaining data from multiple scan angles. This results in reduction of conspicuity of stone and shadow boundaries, leading to errors in size measurements. Harmonic imaging augments imaging by adding data obtained from higher frequencies. This improves lateral resolution and hence results in a more accurate estimate of actual stone size. However, this comes at the expense of signal to noise and depth penetration.
C. Incorrect. The smaller the stone, the greater the error in measurement especially if the stone is <5 mm.
D. Incorrect. Ultrasound tends to overestimate the size of stones.
Question 4.5: A longitudinal view of a transplanted kidney is presented with color and spectral Doppler analysis. What is the diagnosis?

Arteriovenous fistula.
Pseudoaneurysm.
Calculus.
Renal vein thrombosis.
Answer:
A. Correct. The images demonstrate an area of color aliasing within the inferior pole of the transplanted kidney. Spectral Doppler demonstrates high-volume, low-resistance flow with arterial peaks. These findings are consistent with an arteriovenous fistula.
B. Incorrect. Pseudoaneurysms typically demonstrate a yin yang appearance on color Doppler images. On spectral Doppler, there is typically alternating flow above and below the baseline.
C. Incorrect. The “twinkle sign” may be observed with renal calculi and may demonstrate an appearance similar to the color Doppler picture. However, the flow pattern present on spectral Doppler in this patient confirms authentic flow as opposed to artifact.
D. Incorrect. Renal venous thrombosis typically results in reversal of arterial diastolic flow which is not present in this case.
Question 4.6: The images demonstrate an area of color aliasing within the inferior pole of the transplanted kidney. Spectral Doppler demonstrates high-volume, low-resistance flow with arterial peaks. Appropriate initial management of the finding would include?

Embolization.
Injection of sclerosant.
Expectant, as this is typically self-limiting.
Percutaneous nephrostomy.
Answer:
C. Correct. Iatrogenic arteriovenous fistulas are usually self-limiting.
A, B—Incorrect. The condition is self-limiting.
D. Incorrect. This would be inappropriate as there is no evidence of hydronephrosis.
Question 4.7: What is the most likely diagnosis in this adult patient?

Autosomal recessive polycystic kidney disease.
Lupus nephritis.
Normal variant.
Acute pyelonephritis.
Answer:
B. Correct. The kidneys are usually affected in patient with systemic lupus erythematosus. The pathogenesis includes immune complex deposition within glomeruli. Typically, the kidneys demonstrate diffusely increased echogenicity.
A. Incorrect. Autosomal recessive polycystic kidney disease most commonly results in fetal demise. However, when presenting in childhood or adulthood, the kidneys are noted to be enlarged, containing innumerable tiny cysts.
C. Incorrect. This appearance is abnormal in an adult patient.
D. Incorrect. The renal sonogram is typically normal in cases of acute pyelonephritis.
Question 4.8: What is the most likely diagnosis in this adult patient?

Autosomal recessive polycystic kidney disease.
Lupus nephritis.
Medullary sponge kidney.
Pyelonephritis.
Answer:
C. Correct. Medullary sponge kidney is the result of structural abnormality of the collecting tubules. The tubules become ectatic and serve as a point of calculus formation. This is a classic cause of medullary nephrocalcinosis and typically manifests as increased echogenicity of renal medulla.
A. Incorrect. Autosomal recessive polycystic kidney disease most commonly results in fetal demise. However, when presenting in childhood or adulthood, the kidneys are noted be enlarged containing innumerable tiny cysts.
B. Incorrect. The renal cortex is typically hyperechoic in lupus nephritis.
D. Incorrect. The renal sonogram is typically normal in cases of acute pyelonephritis.
Question 4.9: A transplanted kidney is demonstrated below. What is the diagnosis?

Arteriovenous fistula.
Pseudoaneurysm.
Calculus.
Renal vein thrombosis.
Answer:
D. Correct. The spectral waveform demonstrates reversal of arterial diastolic flow. In a transplanted kidney, this is the typical finding in renal vein thrombosis.
A. Incorrect. In the setting of an arteriovenous fistula, spectral Doppler demonstrates high-volume, low-resistance flow with arterial peaks.
B. Incorrect. While spectral Doppler may demonstrate alternating flow above and below the baseline within the neck of a pseudoaneurysm, the typical yin yang appearance of the actually pseudoaneurysm is not present on the color Doppler images.
C. Incorrect. A calculus is not imaged.
Question 4.10: The spectral waveform obtained in this transplanted kidney is presented below, demonstrating reversal of arterial diastolic flow. This finding is typical of renal vein thrombosis. When does this typically occur?

Within the first week post transplant.
Between 1 to 6 months post transplant.
Between 6 to 12 months post transplant.
After a year post transplant.
Answer:
A. Correct. Renal vein thrombosis typically occurs within the first week after transplantation and may be due to local compression from post op fluid collections, hypovolemia and surgical technique.
B, C, D—Incorrect. Renal vein thrombosis typically occurs within the first week after transplantation.
Question 4.11: The lower poles of this patient’s kidneys have been repetitively difficult to demonstrate sonographically. What is the most likely cause?

Too much overlying bowel gas.
Horseshoe kidney.
Multiple shadowing calculi.
Lumbar ribs.
Answer:
B. Correct. One of the most consistent sonographic findings in horseshoe kidney is the inability to adequately demonstrate the lower poles as they deviate medially.
A. Incorrect. Bowel gas would probably not be a repetitive problem in the same area. Also altering the patient’s position and employing different degrees of inspiration would facilitate better viewing of the lower poles.
C. Incorrect. Shadowing calculi would be expected to produce echogenic foci with posterior shadowing, which is not present in this case.
D. Incorrect. Rib shadows originate from the body wall, closer to the near-field, which is not the case in this patient.
Question 4.12: What anatomic structure is indicated by the arrow ?

Gallbladder.
Pylorus.
Right atrium.
Esophagus.
Answer:
C. Correct. The arrow points to the right atrium.
A, B, D—Incorrect. These anatomic structures are not indicated by the arrow.
Question 4.13: At least what T stage of disease do the images in (Question 4.12) reveal, using the TNM classification?
T4.
T3C.
T3B.
T3A.
Answer:
B. Correct. The images demonstrate a rounded mass at the superior aspect of the left kidney with soft tissue material extending to involve the right atrium. These findings are typical of renal cell carcinoma with tumor thrombus extending to the right atrium, that is, above the diaphragm and hence the stage is T3C.
A. Incorrect. Stage T4 represents tumors that have spread beyond Gerota’s fascia.
C. Incorrect. Stage T3B represents cases with tumor thrombus extending within the inferior vena cava but remaining below the diaphragm.
D. Incorrect. Stage T3A represents cases in which the tumor involves the adjacent perinephric fat or adrenal gland.
Question 4.14: This patient likely suffers from which of the following?

Essential hypertension.
Absence seizures.
Type 2 diabetes.
Bipolar disorder.
Answer:
D. Correct. The kidneys demonstrate multiple punctate echogenic foci throughout the parenchyma. These are typical findings of lithium nephropathy and thought to correspond to multiple microcysts throughout the kidney. Lithium is used in the treatment of bipolar disorder.
A, B, C—Incorrect. The findings are due to long-term lithium use.
Question 4.15: This adult patient presents with hematuria. Bilateral renal sonograms are obtained. Which statement is correct?

There is a contour deforming renal mass.
There is left upper pole caliectasis.
There is evidence of right renal artery stenosis.
There is no discernible cause for hematuria on the images provided.
Answer:
B. Correct. Not only is there left upper pole caliectasis, there is also subtle soft tissue material within the calyx. This represents a urothelial neoplasm and the appearance is often termed an “oncocalyx.”
A. Incorrect. No contour deforming mass is present.
C. Incorrect. Renal artery stenosis often presents morphologically as uniformly small kidney. Both kidneys are similar in size.
D. Incorrect. Left upper pole “oncocalyx” is present.
Question 4.16: What underlying condition should be excluded?

Prostate cancer.
Ectopic ureter.
Hydronephrosis.
Renal cell carcinoma.
Answer:
C. Correct. The images demonstrate bladder trabeculation and an enlarged prostate. The findings are consistent with chronic bladder outlet obstruction necessitating the exclusion of obstructive nephropathy.
A. Incorrect. There is no finding to suggest underlying prostate cancer.
B. Incorrect. There is no finding to suggest underlying ectopic ureter.
D. Incorrect. There is no finding to suggest underlying renal cell cancer.
Question 4.17: What is the cause of pain in this 35-year-old female?

Acute appendicitis.
Distal ureteral calculi.
Ovarian vein thrombosis.
Endometriosis.
Answer:
B. Correct. The transvaginal sonogram demonstrates tiny echogenic calculi within the distal ureters (seen in the near-field), a useful albeit fortuitous finding in this patient.
A. Incorrect. The appendix is not imaged.
C. Incorrect. In this image ovarian vein thrombosis is not present.
D. Incorrect. Findings of endometriosis are not imaged.
Question 4.18: This new transplant requires which of the following options?

Reexploration.
Short interval repeat scanning.
A nephrostomy tube.
Urgent pelvic CT with intravenous contrast.
Answer:
A. Correct. The image demonstrates diminished perfusion in the upper pole of the transplanted kidney. This was due to acute occlusion of the upper pole branch of an early bifurcating transplant artery. This was successfully treated with open embolectomy.
B. Incorrect. This would not be helpful and the delay in definitive treatment would further compromise the graft.
C. Incorrect. There is no hydronephrosis.
D. Incorrect. The renal transplant vasculature is adequately evaluated with ultrasound.
Question 4.19: This diabetic patient presents with a history of abdominal pain and compromised renal function. What is the likely diagnosis?

Left nephrectomy.
Medullary nephrocalcinosis.
Xanthogranulomatous pyelonephritis.
Emphysematous pyelonephritis.
Answer:
D. Correct. The left renal image demonstrates irregular echogenic areas within the renal bed with “dirty shadowing” consistent with renal parenchymal gas. In a diabetic patient, these findings are highly suggestive of emphysematous pyelonephritis.
A. Incorrect. There was no history of left nephrectomy.
B. Incorrect. This is not the appearance of medullary nephrocalcinosis which is characterized by increased echogenicity of the medullary pyramids.
C. Incorrect. This is not the sonographic appearance of xanthogranulomatous pyelonephritis which is characterized by an obstructing staghorn calculus within the pelvicalyceal system with hypoechoic, distended calyces.
Question 4.20: A 55-year-old male with a history of renal transplantation 6 years prior, presents with elevated creatinine. Sagittal views of the transplanted kidney are shown below, with color Doppler evaluation of a lesion. Which statement is correct?

The images demonstrate multiple complex fluid collections likely representing abscesses.
The collections are likely to be sterile since renal transplants are not typically predisposed to parenchymal abscess formation due to the relatively short ureter.
The findings are consistent with lymphoceles.
The findings likely represent spontaneous intraparenchymal hemorrhage, a frequent complication of longstanding renal transplants.
Answer:
A. Correct. Recipients of renal transplantation typically experience frequent allograph infections due to immunosuppressive medications, frequent instrumentation, and indwelling catheters. Frequent glycosuria is also a risk factor. Prompt drainage and antibiotics administration is necessary to prevent loss of the transplant.
B. Incorrect. Transplanted kidneys are susceptible to infection.
C. Incorrect. Lymphoceles are typical anechoic and simple in appearance. Occasionally they may contain septations. Also, lymphoceles are usually external to the renal parenchyma.
D. Incorrect. Intraparenchymal hematomas usually result from interventions such as biopsies as opposed to being spontaneous.
Question 4.21: A 48-year-old patient presents for routine sonographic evaluation of her renal transplant. Transverse and sagittal images obtained during the evaluation are demonstrated below. What accounts for this appearance?

Mirror image artifact.
Transplantation of two kidneys.
Fluid collection.
Retained foreign body.
Answer:
B. Correct. The patient underwent en bloc transplantation of both kidneys from a pediatric donor. En bloc transplantation recipients show excellent long-term outcome, with 5-year graft survival similar to living-related donor kidneys.
A, C, D—Incorrect. The appearance is due to two separate kidneys.
Question 4.22: What is the likely cause for low urine output in this female patient with history of abdominal pain?

Bladder leak.
Chronic renal failure.
Hypovolemia.
None of the above.
Answer:
D. Correct. The sonographic image demonstrates inadvertent malpositioning of the urethral catheter with the catheter balloon inflated within the vagina.
A. Incorrect. A bladder leak would manifest as pelvic free fluid.
B, C—Incorrect. The urethral catheter is malpositioned.
Question 4.23: What is the likely etiology of this fluid collection (blue arrow) in this diabetic male patient with a remote history of a renal transplant? The urinary bladder is indicated by the yellow arrow.

Urinoma.
Foreign body.
Abscess.
Artifact.
Answer:
B. Correct. This well-defined fluid-filled structure corresponds to the reservoir of a penile prosthesis device. Diabetic patients may suffer from erectile dysfunction as well as renal failure, thus this “fluid collection” should be entertained in men with renal transplantation.
A. Incorrect. Urinomas are uncommon and usually present early after transplantation.
C. Incorrect. An abscess typically presents as a complex fluid collection.
D. Incorrect. The well-defined fluid-filled structure corresponds to the reservoir of a penile prosthesis device.
Question 4.24: A left ureteral jet is observed. What accounts for this phenomenon?

The Doppler shifts are mostly created by particulate debris within urine.
Differences in specific gravity between ureteral and bladder urine allow detection of the jet.
Changes in abdominal cavity pressure with respiration.
Changes in abdominal cavity pressure with Valsalva.
Answer:
B. Correct. Observed ureteral jets are at least partly due to the differences in specific gravity of “incoming” ureteral urine and long-standing urine within the bladder. Ureteral jets are less apparent if the bladder is quickly filled from empty, say by aggressive hydration, since the incoming ureteral urine and bladder urine would be in similar specific gravity.
A. Incorrect. Particulate debris may be seen in cases of urinary tract infections but does not account for ureteral jets.
C, D—Incorrect. These options does not account for ureteral jets.
Question 4.25: The right ureteral jet was not observed in this patient after 1 minute of continuous scanning. Which statement is correct?

In the correct clinical context, an obstructing right ureteral calculus is likely present.
In the correct clinical context, a ureteral injury is likely present.
All of the above.
None of the above.
Answer:
D. Correct. None of the above. The rates at which ureteral jets are observed in normal volunteers vary greatly. One minute of observation is not sufficient to assume obstruction. Most protocols advocate for at least a 5-minute period of observation.
A, B, C—Incorrect. One minute of observation is not sufficient to assume ureteral obstruction. Most protocols advocate for at least a 5-minute period of observation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


