Chapter 8 Neck
Adrian Dawkins
8 Questions and Answers
Refer to the following figure for questions 8.1 and 8.2.

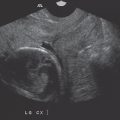
Question 8.1 This 35-year-old patient is scheduled for a barium swallow within the radiology department. During the study, the patient aspirates barium. Which structures will be opacified by barium?
A and B.
A and C.
B and C.
B and D.
Question 8.2: What frequency is typically employed in the sonographic evaluation of neck structures?
2 to 3 MHz.
3 to 5 MHz.
5 to 12 MHz.
30 to 35 MHz.
Answer 8.1:
C. Correct. This high-resolution sonographic image depicts a transverse view of the neck at the level of the thyroid gland. The butterfly-shaped thyroid gland is seen as a smooth fairly echogenic structure with right (A) and left lobes connected by the midline isthmus which is positioned anterior to the trachea (B). In the supine position, the esophagus (C) is frequently identified as a circular structure with several layers just the left and posterior to the trachea. The layered appearance of the esophagus is due to the differing echogenicities of wall components. The curved reflective surface of a cervical vertebral body (yellow arrow) is noted posterior to the trachea. Paired strap (star) and longus colli muscles (D) are also noted.
A. Incorrect. This represents the right lobe of the thyroid and trachea respectively.
B. Incorrect. This represents the right lobe of the thyroid and the esophagus respectively.
D. Incorrect. This represents the trachea and the longus colli muscle respectively.
Answer 8.2:
C. Correct. The superficial location of neck structures as well as large surface area of overlying skin, allow sonographic evaluation at high frequencies using a linear transducer. The resulting image is typically of high resolution, optimal for discerning anatomy and pathology, as well as guiding interventions.
A. Incorrect. This frequency range is typically employed for abdominopelvic scanning, particularly in obese patients, due to better penetration of the low frequency sound beam.
B. Incorrect. This frequency range is typically employed for abdominopelvic scanning.
D. Incorrect. This frequency range is not typically used in medical imaging.
Question 8.3: This image is obtained from a submental view of the neck. What structures are labeled A, B, and C?

Mylohoid muscle, submandibular gland, and anterior belly of the diagastric muscle respectively.
Mylohoid muscle, submandibular gland, and the tongue respectively.
Anterior belly of the digastric muscle, sublingual gland, and the tongue respectively.
Anterior belly of the digastric muscle, submandibular gland, and the tongue respectively.
Answer:
C. Correct. The submental view is easily acquired by positioning the transducer in such a way that the footprint of the probe contacts the skin beneath the chin. The resulting image, when the probe is held transverse, is an “upside down coronal view” of the face. The anterior bellies of the digastric muscles (A) are seen as paired superficial structures. The mylohyoid muscle (yellow arrow) is seen as a superficial diaphragm-like muscle forming the floor of the mouth. Deep to this, the tongue is seen as a midline collection of several muscle bellies (C) with the echogenic sublingual glands (B) on either side. The image is classic and typically symmetric.
A. Incorrect. The mylohyoid muscle is indicated by the yellow arrow. The submandibular glands are not imaged. The anterior belly of the digastric muscle is indicated by (A).
B. Incorrect. The mylohyoid muscle is indicated by the yellow arrow. The submandibular glands are not imaged. The tongue is indicated by (C).
D. Incorrect. The anterior belly of the digastric muscle is indicated by (A). The submandibular glands are not imaged. The tongue is indicated by (C).
Question 8.4: The sonographic image below represents a longitudinal midline view of the neck. What structure is labeled A and B?

Thyroid cartilage and the thyroid isthmus.
Thyroid isthmus and the cricoid cartilage.
Thyroid cartilage and the cricoid cartilage.
Cricoid cartilage and a tracheal ring.
Answer:
C. Correct. This sonographic image is readily obtained by placing the transducer within the midline of the neck in the longitudinal plane. Ample ultrasound gel is required to maintain skin contact. The repetitive tracheal cartilaginous rings (yellow arrow) are noted as hypoechoic structures along the length of the trachea. The long slender echogenic line running along the trachea represents the highly reflective air that occupies the tracheal lumen. The cricoid cartilage is a larger, circumferentially complete cartilaginous ring at the cranial aspect of the trachea. The thyroid cartilage is seen as a larger hypoechoic structure at the cranial aspect of the image. The cricothyroid membrane occupies the space between the thyroid and cricoid cartilages and serves as the site for a cricothyroidotomy, an airway rescuing procedure.
A, B—Incorrect. The thyroid isthmus is not well-depicted but would be expected to be hyperechoic, overlying the tracheal cartilages.
D. Incorrect. Tracheal rings are illustrated by the yellow arrow.
Refer to the following figure for questions 8.5 to 8.7.

Question 8.5: Patient A is 57-year-old female who complains of voice changes. Neck ultrasound reveals enlargement of the left lobe of the thyroid gland. Compression at what point likely accounts for her symptoms?
A.
B.
C.
D.
Question 8.6: Patient B demonstrates a lesion (yellow arrow) that splays the internal jugular vein (IJV) (compressed) and the common carotid artery (blue arrow). From which structure does it likely arise?
Accessory spinal nerve.
Recurrent laryngeal nerve.
Vagus nerve.
Hypoglossal nerve.
Question 8.7: What underlying pathology best accounts for the finding in patient B?
Sturge–Weber syndrome.
Follicular thyroid cancer.
Neurofibromatosis.
Sarcoidosis.
Answer 8.5:
B. Correct. The recurrent laryngeal nerve (branch of the vagus nerve) runs in space between the trachea and medial aspect of the thyroid lobes. It provides motor supply to the vocal cords. Enlargement of the thyroid may result in compression of the recurrent laryngeal nerve, leading to hoarseness.
A. Incorrect. (A) represents the trachea.
C. Incorrect. (C) represents the substance of the enlarged left lobe of the thyroid.
D. Incorrect. (D) represents the carotid sheath containing the internal jugular vein, common carotid artery, and the vagus nerve.
Answer 8.6:
C. Correct. The vagus nerve runs within the carotid sheath along with the IJV and common carotid artery.
A. Incorrect. This not the anatomic location of the accessory spinal nerve.
B. Incorrect. This not the anatomic location of the recurrent laryngeal nerve.
D. Incorrect. This not the anatomic location of the hypoglossal nerve.
Answer 8.7:
C. Correct. Patient B is known to have neurofibromatosis type 2 with multiple nerve sheath tumors including the one in this case. The location of the lesion predicts its neural origin.
A. Incorrect. Sturge–Weber syndrome is characterized by port-wine stains involving the face and angiomas of the pia mater. There is an association with paragangliomas which technically include glomus vagale tumors. However, these typically occur at the common carotid bifurcation, splaying the internal and external carotid arteries. This rather tenuous link is, therefore, not the correct option.
B. Incorrect. Follicular thyroid cancer typically metastasizes via the hematogenous route. Hence regional lymphadenopathy is not the best choice. On the other hand, papillary thyroid cancer frequently metastasizes via the lymphatics.
D. Incorrect. Sarcoidosis is a systemic disease characterized by noncaseating granulomas. Nodal disease typically involves the bilateral hilar and paratracheal regions. While cervical lymphadenopathy is possible, this is not the typical site.
Refer to the following figure for questions 8.8 to 8.10.

Question 8.8: This transverse submental view obtained from patient A demonstrates asymmetry. What is the likely diagnosis?
Thyroglossal duct cyst.
Lingual thyroid.
Metastatic disease.
Second branchial cleft cyst.
Question 8.9: This longitudinal midline view of the neck, at the level of the hyoid bone (yellow arrow), was obtained in patient B. This patient was suspected to have thyroid cancer recurrence based on a radioiodine scan. What explains this finding?
Lymphangioma.
Thyroglossal duct cyst.
Recurrent thyroid cancer.
Ranula.
Question 8.10: What maneuver may assist with the diagnosis in patient B?
Erect and supine posture.
Lateral decubitus positioning.
Tongue protrusion.
Valsalva.
Answer 8.8:
C. Correct. Patient A has biopsy-proven squamous cell carcinoma at the base of the tongue. The lesion with the left aspect of the floor of the mouth represents a metastatic deposit.
A. Incorrect. A thyroglossal duct cyst is a fluid-filled cavity occurring along the path of embryologic decent of the thyroid. It is typically midline in location and may contain ectopic thyroid tissue. This lesion typically elevates on tongue protrusion.
B. Incorrect. A lingual thyroid occurs typically when normal descent of the thyroid gland from the base of the tongue to the mid neck does not occur. Most often, the ectopic thyroid gland is entirely located at the base of the tongue, within the midline, with no thyroid tissue demonstrable within the usual pretracheal location. This image demonstrates a small, hypoechoic lesion far away from midline.
D. Incorrect. A second branchial cleft cyst is a developmental anomaly resulting in the formation of a cystic lesion which is typically located anterior to sternocleidomastoid muscle.
Answer 8.9:
B. Correct. Patient B demonstrates the classic appearance and location of a thyroglossal duct cyst. As already mentioned, a thyroglossal duct cyst is fluid-filled cavity occurring along the path of embryologic decent of the thyroid. It is typically midline in location and may contain ectopic thyroid tissue. This accounts for the activity seen on thyroid tissue sensitive nuclear medicine studies.
A. Incorrect. A lymphangioma is a benign fluid-filled lesion occurring typically around the head and neck in the pediatric population. They are also known as cystic hygromas and tend to contain septations.
C. Incorrect. Recurrent thyroid cancer does not typically manifest as a purely cystic lesion.
D. Incorrect. A ranula is a type of retention cyst usually occurring in the sublingual space, off mid-line, as a result of sublingual glandular infection or trauma.
Answer 8.10:
C. Correct. The attachment of the thyroglossal duct cyst to the base of the tongue results in elevation of the lesion on tongue protrusion.
A, B, D—Incorrect. These maneuvers would not be helpful.
Refer to the following figure for questions 8.11 to 8.13.

Question 8.11: This sonographic image of the left parotid gland of a 55-year-old chronic smoker demonstrates an abnormality. What is the most likely diagnosis?
Pleomorphic adenoma.
Warthin tumor.
Parotid cyst.
Hemangioma.
Question 8.12: The above lesion was biopsied. Which of the following clinical manifestations suggests nerve injury?
Ipsilateral face droop and forehead paralysis.
Contralateral face droop and forehead paralysis.
Contralateral face droop and preserved forehead motor function.
Ipsilateral face droop and preserved forehead motor function.
Question 8.13: A Tc-99m pertechnetate scan was undertaken for another unrelated indication. Incidental observations were made with regard to the parotid lesion. Which of the following is true?
A cold lesion excludes benignity.
A hot lesion is most often malignant.
A hot lesion is suggestive of Warthin tumor.
Tc-99m pertechnetate is useful in differentiating the different types of parotid malignancies.
Answer 8.11:
B. Correct. Warthin tumors are the second most common benign tumors of the parotid gland, behind pleomorphic adenomas. Warthin tumors are slow-growing and occur typically in middle-aged men with a history of smoking. They are hypoechoic on ultrasound with occasional cystic spaces. Posterior acoustic enhancement may also be present. The appearance and location of the lesion, coupled with the history, make option B the correct choice.
A. Incorrect. Given the clinical context, option A is incorrect. However, pleomorphic adenomas may share some sonographic features with the Warthin tumor.
C. Incorrect. Parotid cysts are uncommon. When present, they are typically well-defined and anechoic.
D. Incorrect. Parotid hemangiomas typically occur in the pediatric population. They may contain phleboliths, typically seen as punctate echogenic foci.
Answer 8.12:
A. Correct. Facial nerve injury is uncommon during parotid fine needle aspiration (FNA). If injury or compression of the nerve ensues, say from a large intraparotid hematoma or subsequent abscess, this may manifest as a lower motor neuron type injury characterized by ipsilateral face droop and ipsilateral forehead paralysis. Recall, the facial nerve gives rise to five terminal branches within the parotid gland, which supply the muscles of facial expression. Insults occurring proximal to the brainstem result in contralateral facial droop and preservation of forehead motor function due to cross-over/dual forehead innervation at this level.
B, C, D—Incorrect. These are not the signs of a lower motor neuron injury.
Answer 8.13:
C. Correct. Parotid malignancies manifest as cold lesion on Tc-99m pertechnetate studies. Pleomorphic adenomas are also “cold” on this study which helps to differentiate them from a Warthin tumor which is typically hot due to an abundance of mitochondria within oncocytes.
A, B, D—Incorrect. These options are incorrect due to the above mentioned reason.
Refer to the following figure for questions 8.14 to 8.16.

Question 8.14: This transverse image of the right cheek, taken at the level of the upper maxilla demonstrates what pathology?
Sialolithiasis.
Thrombophlebitis.
Cellulitis.
Sialadenitis.
Question 8.15: This pathology is encountered most frequently in which location?
Parotid glands.
Sublingual glands.
Submandibular gland.
Accessory salivary glands.
Question 8.16: What is the term for sialadenitis due to ductal obstruction from a mucus plug?
Kussmaul disease.
Kuttner’s tumor.
Kimura’s disease.
Mikulicz’s disease.
Answer 8.14:
A. Correct. The image demonstrates distention of the main duct of the parotid gland, also known as Stensen’s duct. With the duct there are several calculi, the largest of which sits just inferior to the body maker at the upper left corner of the image. Sialolithiasis is the second most common cause of sialadenitis next only to mumps.
B. Incorrect. The imaged tubular structure is the main parotid duct, not a vein.
C. Incorrect. There are no imaging features to support this diagnosis.
D. Incorrect. The actual parotid gland is not imaged. Hence, a diagnosis of sialadenitis cannot be made on the basis of this image.
Answer 8.15:
C. Correct. Sialolithiasis is very common in the submandibular gland and may cause diffuse or focal enlargement of the gland. Thick, alkaline saliva coupled with the uphill course of Wharton’s duct (main duct of the submandibular gland) may account for this observation.
A, B, D—Incorrect. Sialolithiasis most frequently affects the submandibular gland.
Answer 8.16:
A. Correct. Kussmaul disease (sialodochitis fibrinosa) is described as an acute episode of sialadenitis secondary to obstruction of the main duct.
B. Incorrect. A “Kuttner’s tumor” describes a palpable firm, mass-like submandibular gland due to chronic inflammation.
C. Incorrect. Kimura’s disease is a chronic inflammatory disease of the cervical lymph nodes and salivary glands. It is characterized by eosinophilia and markedly elevated serum IgE. It typically afflicts Asian males.
D. Incorrect. Mikulicz’s syndrome is a variant of Sjogren’s syndrome characterized by inflammation of two or more salivary and lacrimal glands. Xerostomia is also present.
Question 8.17: The cystic lesions of the parotid gland shown below in patient A are most commonly encountered with which pathogen?

Cytomegalovirus.
Human immunodeficiency virus (HIV).
Hepatitis B virus.
Mycobacterium tuberculosis.
Answer:
B. Correct. Patient A demonstrates multiple cystic lesions throughout the parotid gland. These findings are typical of benign lymphoepithelial lesions, a frequent finding in patients with HIV infection. The parotid glands are most frequently affected and there is an association with cervical lymph node enlargement.
A. Incorrect. Cytomegalovirus is not associated with parotid cysts.
C. Incorrect. Hepatitis B virus is not associated with parotid cysts.
D. Incorrect. Mycobacterium tuberculosis is not associated with parotid cysts.
Question 8.18: Patient B is a 31-year-old female. A sonographic image of one of her parotid glands is presented. Which of the following is true?

The findings are consistent with Sjogren’s disease.
The findings are within normal limits.
This appearance should prompt a thorough search for intraparotid lymph nodes, since lymph nodes in the parotid gland are usually abnormal.
None of the above.
Answer:
A. Correct. This image was obtained from an adult female patient with Sjogren’s disease. The typical sonographic appearance includes multiple hypoechoic foci throughout the gland correlating with aggregates of lymphocytes.
B. Incorrect. The normal parotid gland typically demonstrates smooth echotexture and is homogenously echogenic.
C. Incorrect. While there is an increased risk of developing Non-Hodgkin’s lymphoma in patients with Sjogren’s disease, intraparotid lymph nodes are normal findings. Late embryologic encapsulation results in normal lymph nodes being incorporated within the parotid.
D. Incorrect.
Question 8.19: In this sonographic image, which structure is represented by the yellow arrow ?

An abnormal lymph node.
A normal variant.
A normal lymph node.
None of the above.
Answer:
B. Correct. The arrow indicates an accessory parotid gland, a normal variant. Typically, the accessory gland is located anterior to the main parotid gland and derives its separate blood supply from the transverse facial artery. It drains via a separate duct to the main parotid duct. Any pathology affecting the parotid glands can also affect the accessory parotid.
A. Incorrect. This accessory parotid gland demonstrates a smooth, homogenously echogenic appearance, identical to the main parotid gland. This would be an unusual appearance for a lymph node, normal or abnormal.
C. Incorrect. A normal lymph node is typically reniform and demonstrates an echogenic hilum. These findings are not present.
D. Incorrect.
Question 8.20: Based on the images below, what likely accounts for the abnormal appearance of the submandibular glands of this 35-year-old male patient?

Therapeutic radioiodine changes 5 years after treatment.
Sjogren’s disease.
Parvovirus infection.
Sarcoidosis.
Answer:
D. Correct. The images demonstrate normal parotid glands and with enlarged, heterogeneously hypoechoic submandibular glands. Sarcoidosis may involve both the parotid and submandibularglands. However, sole submandibular gland involvement is more frequent than sole parotid involvement.
A. Incorrect. The submandibular glands are frequently affected by radiotherapy-induced changes secondary to thyroid malignancy treatment. However, after a few years, the glands are usually relatively atrophic and small as opposed to enlarged as seen in this case.
B. Incorrect. Sjogren’s syndrome is a chronic autoimmune disorder affecting the lacrimal and salivary glands. Patients typically demonstrate, dry eyes, dry mouth, and bilateral parotid swelling. On ultrasound the parotid glands are noted be enlarged with varying echogenicity, hyperechoic in the early stages and hypoechoic/multicystic later on in the disease course.
C. Incorrect. Parvovirus infection (mumps) typically affects the parotid gland.
Refer to the following figure for questions 8.21 and 8.22.

Question 8.21: This longitudinal sonographic view of the left lobe of the thyroid demonstrates a rounded thyroid lesion. Which option is consistent with appropriate management?
FNA.
Thorough neck ultrasound to exclude a primary malignancy.
Antibiotics.
No further action required.
Question 8.22: What type of artifact is demonstrated by the yellow arrow in the image?
Reverberation.
Mirror image.
Shadowing.
Side lobe.
Answer 8.21:
D. Correct. The image demonstrates a well-defined almost purely cystic lesion with a contained echogenic focus demonstrating a “comet tail.” This is the classic appearance of a colloid cyst, a benign entity requiring no further management.
A. Incorrect. Colloid cysts are benign and do not require FNA.
B. Incorrect. Colloid cysts are benign. They are not associated with malignancies.
C. Incorrect. Antibiotics would be inappropriate as there is no underlying infection.
Answer 8.22:
A. Correct. The arrow indicates an echogenic focus with an associated “comet tail,” commonly referred to as comet tail artifact. This is a type of reverberation artifact caused by sound “bouncing” back and forth between two closely spaced reflective surfaces. Pure reverberation artifact results in a repetitive display of equally spaced echogenic lines. However, for comet tail artifact, the echogenic lines are so close together that they are perceived as one entity. The later (and hence deeper) echoes are more attenuated and thus are displayed with diminished widths, leading to the tapered or triangular appearance.
B. Incorrect. Mirror image artifact is also due to multiple reflections of the primary ultrasound beam usually from a highly reflective surface deep to the duplicated structure. The mirror image is displayed at an equal distance on the opposite side of the reflector.
C. Incorrect. Shadowing occurs when transmission of sound through a structure is poor relative to the adjacent structures resulting in a dark band or “shadow” deep to the imaged structure.
D. Incorrect. Side lobes are weak off-axis ultrasound beams. If they encounter a very strong reflector which is lateral to the main scan line, the reflector may be erroneously placed within the path of the main scan line. This artifact is more obvious when an anechoic structure occupies the main scan line, such as a full urinary bladder.
Refer to the following figure for questions 8.23 to 8.25.

Question 8.23: What unique entity does this ill-defined lesion within the right lobe of the thyroid likely contain?
Koilocytes.
Parafollicular C cells.
Hurthle cells.
Psammoma bodies.
Question 8.24: In general, what sonographic feature is felt to predict malignancy in thyroid nodules?
Wider than tall.
Very hyperechoic.
Ill-defined margins.
Solid composition.
Question 8.25: The above lesion was biopsied. Which specimen is deemed adequate?
Little to no blood within the specimen and four follicular groups.
At least six follicular groups.
At least five follicular groups and the absence of ultrasound gel within the specimen.
Scant colloid and at least four follicular groups.
Answer 8.23:
D. Correct. Psammoma bodies are tiny areas of lamellated calcification. These are frequently encountered in papillary carcinoma of the thyroid and manifest as multiple tiny echogenic foci.
A. Incorrect. Koilocytes are associated with human papillomavirus infection.
B. Incorrect. Parafollicular C cells are the site of origin of medullary thyroid cancer.
C. Incorrect. Hurthle cells are typically associated with Hashimoto’s thyroiditis or a variant of follicular thyroid carcinoma.
Answer 8.24:
D. Correct. The relatively new thyroid imaging reporting and data system (TIRADS) classification scores thyroid nodules with respect to composition, margin, echogenicity, shape, and echogenic foci. The points allocated for each category are summated and the higher the score, the greater the likelihood of malignancy. A solid or predominately solid nodule scores 2 points, the highest for the “composition category.”
A. Incorrect. A taller than wide nodule is more suspicious than vice versa and scores maximum (3 points) for the “shape” category.
B. Incorrect. A very hypoechoic nodule scores the maximum of 3 points for the “echogenicity” category.
C. Incorrect. Though somewhat counterintuitive, a nodule with ill-defined margins actually scores zero for the “margin” category. A lobulated or irregular margin scores 2 points whereas extrathyroid extension scores 3.
Answer 8.25:
B. Correct. A thyroid nodule FNA sample is deemed adequate if there are 6 well-preserved groups of follicular cells, each containing at least 10 cells.
A, C, D—Incorrect. These are not deemed adequate.
Refer to the following figure for questions 8.26 to 8.28.

Question 8.26: Sonographic images of the thyroid gland are shown above. What is the most likely diagnosis?
Graves’ disease.
Hashimoto’s thyroiditis.
Lymphoma.
Thyroid abscess.
Question 8.27: What further abnormality is probably present?
Antithyroglobulin antibodies.
Elevated T3 and T4.
Neck pain and preceding history of a viral infection.
IgG4-related sclerosing disease.
Question 8.28: Which of the following is employed in the diagnosis of this disease?
123I-NaI.
123I-meta-iodobenzylguanidine (123I-MIBG).
123I-DaTscan.
None of the above.
Answer 8.26:
A. Correct. Graves’ disease is an autoimmune disease affecting the thyroid gland caused by antibodies that target thyroid-stimulating hormone (TSH) receptors. On ultrasound, the gland is swollen and diffusely hypoechoic. Color Doppler demonstrates markedly increased vascularity described as “thyroid inferno.” These features are demonstrated in the provided images.
B. Incorrect. Hashimoto’s thyroiditis is typically characterized by an enlarged hypoechoic gland with heterogeneous echotexture with bright fibrotic bands. Vascularity on color Doppler is variable and, while thyroid inferno may rarely occur, it is more likely to be associated with Graves’ disease.
C. Incorrect. Thyroid lymphoma typically presents as a heterogeneously enlarged thyroid without normal intervening parenchyma. Extracapsular extension may also be present. The most common type of thyroid lymphoma is mucosa-associated lymphoid tissue lymphoma, followed by diffuse large B-cell lymphoma. Patients may present with obstructive symptoms due to compression of the airways.
D. Incorrect. A thyroid abscess is an infrequent complication of thyroiditis or other neck inflammatory process. Like abscesses elsewhere in the body, it is characterized by a hypoechoic fluid collection with peripheral hyperemia.
Answer 8.27:
B. Correct. Graves’ thyroiditis is an autoimmune disorder characterized by thyrotoxicosis with an observed increase in both T3 and T4 levels. TSH levels are suppressed.
A. Incorrect. Antithyroglobulin antibodies are typically encountered in Hashimoto’s thyroiditis.
C. Incorrect. Neck pain and preceding history of a viral infection are associated with De Quervain’s thyroiditis.
D. Incorrect. IgG4-related sclerosing disease is associated with Riedel’s thyroiditis. Examples of IgG4-related sclerosing disease include autoimmune pancreatitis and sclerosing mesenteritis.
Answer 8.28:
A. Correct. 123I-NaI scan and uptake are the standard exams to assess patients with Graves’ disease. 123I-NaI has a half-life of 13.22 hours and emits gamma radiation with a 159-keV energy peak, which is suitable for medical imaging. It also allows for uptake measurements which is used for subsequent therapeutic dosage determination.
B. Incorrect. 123I-MIBG is a norepinephrine analogue that is used for the assessment and staging of patents with neuroblastoma and pheochromocytoma but not Grave’s disease, although labelled with 123I.
C. Incorrect. 123I-DaTscan is a cocaine analogue with high affinity to dopamine transporter (DaT) located on the presynaptic nerve endings in the striatum. It is clinically used to differentiate essential tremor from Parkinsonian syndromes. It is also one of the 123I-labelled radiopharmaceuticals that is not used for assessment of Grave’s disease.
D. Incorrect. 123I-NaI is useful in the work-up of patients with Graves’ disease.
Refer to the following figure for questions 8.29 and 8.30.

Question 8.29: Sagittal view of the right lobe of the thyroid gland in a patient with neck fullness. What additional clinical symptom(s) may be present?
Dysphagia.
Heat intolerance.
Rigors and malaise.
Constipation.
Question 8.30: What recommendation should be made to the referring clinician as the logical next step in management of the patient?
Positron emission tomography/computed tomography (PET/CT) from head to mid-thigh to evaluate for primary malignancy.
FNA.
Serum biochemical analysis.
Course of antibiotics.
Answer 8.29:
D. Correct. The ultrasound image demonstrates a well-defined hypoechoic structure along the posterior surface of the thyroid gland. This is the classic appearance of a parathyroid adenoma. The ensuing hyperparathyroidism leads to hypercalcemia and the classic “stones, painful bones, psychic moans and intestinal groans” (hypercalcemia-induced constipation).
A. Incorrect. Dysphagia may be associated with a goitrous enlargement of the thyroid.
B. Incorrect. Heat intolerance is associated with hyperthyroidism.
C. Incorrect. Rigors and malaise suggest underlying infection.
Answer 8.30:
C. Correct. Parathyroid hormone levels and serum calcium may be increased.
A. Incorrect. PET/CT would be inappropriate as there is no underlying malignancy.
B. Incorrect. FNA of a parathyroid adenoma can be helpful by determining the presence of parathormone (PTH) within the aspirate. However, parathyroid FNA can lead to extensive fibrosis, thus rendering surgical excision challenging. Also, the associated fibrosis may be confused with malignancy at histology. Consequently, FNA of parathyroid adenomas is typically avoided in some centers.
D. Incorrect. A course of antibiotic would be inappropriate.
Refer to the following figure for questions 8.31 and 8.32.

Question 8.31: You are reviewing this image of a midline transverse view of the submental region with the ultrasound technologist. The patient is in the scanning room. What should be the next step in imaging?
FNA after contacting the referring service.
No further imaging/workup is required as the finding is clearly benign.
A contrast-enhanced CT of the neck is highly recommended while the patient is still within the radiology department.
None of the above.
Question 8.32: At what level in the neck is the lesion?
Level 1.
Level 2.
Level 3.
Level 4.
Answer 8.31:
D. Correct. This submental nodule is rounded and very hypoechoic. Though it may appear cystic, the lesion actually demonstrated internal vascular flow on color Doppler imaging. Therefore, the next step should be to further evaluate with color Doppler.
A. Incorrect. After evaluating with Doppler, FNA would be appropriate.
B. Incorrect. The lesion was eventually biopsied and confirmed to be lymphoma.
C. Incorrect. A CT of the neck may be appropriate later on in the workup.
Answer 8.32:
A. Correct. Head and neck surgeons as well as pathologists use a simplified numeric classification system to reproducibly identify the locations of cervical lymph nodes. Level 1 lymph nodes are located beneath the chin within the submental or submandibular regions. Quite often, a lymph node is located between the anterior bellies of the digastric muscles, as is the case in this patient with lymphoma.
B. Incorrect. A level 2 lymph node is situated within the internal jugular/deep cervical chain from the level of the skull base to the inferior border of the hyoid bone.
C. Incorrect. A level 3 lymph node is situated within the internal jugular/deep cervical chain from the level of the hyoid bone to the cricoid.
D. Incorrect. A level 4 lymph node is situated within the internal jugular/deep cervical chain from the level of the cricoid to the supraclavicular fossa.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


