Chemotherapeutic Agents from the Perspective of the Radiation Biologist
Chemotherapeutic Agents from the Perspective of the Radiation Biologist
Alice: There’s no use trying—one can’t believe impossible things.
The Queen: I dare say you haven’t had much practice. Why, sometimes I’ve believed as many as six impossible things before breakfast.
—Alice in Wonderland (Lewis Carroll)
This chapter is included after much thought and some equivocation. It was written in response to numerous requests that chemotherapeutic agents be compared and contrasted with radiation from the perspective of the experimental biologist. Many of the techniques and concepts used in chemotherapy were developed initially by radiation biologists, including quantitative tumor assay systems, the concept of cell cycle, sensitivity changes through the cell cycle, and, particularly, population kinetics. The term growth fraction, for example, was coined by a radiation biologist, but never assumed the importance in radiotherapy that it has in chemotherapy.
The study of chemotherapeutic agents in the laboratory, as well as in the clinic, is vastly more complicated than the study of ionizing radiations. For example, dose is more difficult to define or to measure, and time of drug exposure is a critical parameter. Variations in sensitivity through the cell cycle are more dramatic for chemicals than for radiation, assuming essentially an all-ornothing effect for some agents; there are many more factors involving the microenvironment that can influence cellular response.
The term chemotherapy was coined by Paul Erhlich around the turn of the 20th century to describe the use of chemicals of known composition for the treatment of parasites. Erhlich synthesized an organic arsenic compound that was effective against trypanosome infections and rabbit syphilis. This was the first synthetic chemical effective in the treatment of parasitic disease and was rather optimistically named salvarsan, which roughly translates to “the savior of mankind.” The next milestone was the discovery and clinical use of penicillin in the early years of World War II. Alkylating agents had been developed as military weapons by both belligerents in World War I, but it was an explosion in Naples harbor and the exposure of seamen to these agents during World War II that led to the observation that these agents cause marrow and lymphoid hypoplasia. As a result, they were first tested in humans with Hodgkin disease in 1943 at Yale University.
It has long been known beyond doubt that a single chemotherapeutic drug, used in the appropriate schedule, can cure patients with certain rapidly proliferating cancers. The initial demonstration of this was the use of methotrexate to cure patients with choriocarcinoma and, later, the use of cyclophosphamide for Burkitt lymphoma.
The next major step forward was the use of combination chemotherapy in the treatment of acute lymphocytic leukemia in the early 1960s and, subsequently, in the treatment of Hodgkin disease, diffuse histiocytic lymphoma, and testicular cancer in the mid-1970s. These trials verified that multiple non-cross-resistant drugs with different dose-limiting normal tissue toxicities could be used effectively in combination to cure tumors that were not curable with a single agent. The principle of combination therapy was then extended to combined modality treatment, in which chemotherapy was used in conjunction with surgery or radiotherapy, or both, to cure tumors such as pediatric sarcomas.
Today, various antineoplastic agents are used routinely in clinical oncology. Drug-induced cures are claimed for choriocarcinoma, acute lymphocytic leukemia of childhood, other childhood tumors, Hodgkin disease, certain non-Hodgkin lymphomas, and some germ cell tumors of the testes. Other evidence suggests that chemotherapeutic agents given in an “adjuvant” setting for clinically inapparent micrometastatic disease may prolong disease-free survival and possibly effect cure of breast cancer and osteogenic sarcoma.
There are about 13 types of cancer for which cures are claimed by chemotherapy; this accounts for about 10% of all cancers. For comparison, the proportion of cancer patients cured by radiation therapy often is claimed to be about 12.5%. This comes from the so-called 1/2 × 1/2 × 1/2 rule; that is, one-half of all cancer patients receive radiation therapy, one-half of those treated are treated with intent to cure, and one-half of those treated definitively are cured.
The bad public image of chemotherapy relates in large part from the toxicity to normal tissue resulting from multidrug protocols used to induce remissions and achieve tumor cure. “The dose makes the poison” was the advice of Paracelsus, the 16th-century German-Swiss physician and alchemist who established the role of chemistry in medicine. In other words, anything powerful enough to help also has the power to harm. In the past, the lack of tumorspecific agents carried the burden of damage to self-renewing normal tissues, such as the gut and bone marrow. There is hope that the situation is improving with the development of targeted therapies and the new concept of synthetic lethality. (Both will be discussed later in this chapter.)
▪ BIOLOGIC BASIS OF CHEMOTHERAPY
Most anticancer drugs work by affecting DNA synthesis or function, and they usually do not kill resting cells unless such cells divide soon after exposure to the drug. Consequently, the effectiveness of anticancer drugs is limited by the growth fraction of the tumor—that is, by the fraction of cells in active cycle. Rapidly growing neoplasia with a short cell cycle, a large proportion of cells in S phase, and, therefore, a large growth fraction are more responsive to chemotherapy than large tumor masses in which the growth fraction is small. There is a strong tendency for growth fraction to decrease as tumor size increases, at least in experimental animal tumors.
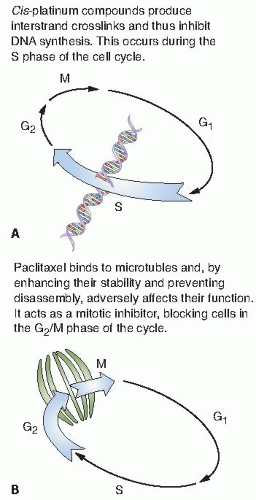
Agents that are mainly effective during a particular phase of the cell cycle, such as S phase or M phase, are said to be cell cycle specific, or phase specific. Those whose action is independent of the position of the cell in the cycle are said to be cell cycle nonspecific or phase nonspecific. Figure 27.1 illustrates two contrasting cell cycle specific drugs. Cis-platinum compounds produce interstrand crosslinks and thus inhibit DNA synthesis; this occurs in S phase. Taxanes bind to microtubules and, by enhancing their stability and preventing disassembly, adversely affect their function. They act as mitotic inhibitors, blocking cells in the G2/M phase of the cell cycle.
Agents that are most effective against cells in S phase are relatively ineffective against cell populations that turn over slowly and have large proportions of dormant cells. On the other hand, the action of alkylating agents and other drugs interacting primarily with macromolecular DNA is largely independent of the phase of the cell cycle, and they may be effective against tumors with relatively low proliferative activity.
The other side of the coin is that the selective normal tissue toxicity of anticancer drugs is reflected in cytotoxic effects on stem cells of the intestinal epithelium or hematopoietic stem cells, which have high growth fractions.
Although many clinical oncologists claim that their thinking has been influenced by research on tumor growth kinetics, it is hard to point to clear advances in treatment that may be attributed to anything more than inspired clinical experimentation. This may be because the study of growth kinetics in human tumors is still in its infancy.
FIGURE 27.1 Two contrasting chemotherapy agents that are both cell cycle specific but produce their effects at quite different phases. A:Cis-platinum compounds produce DNA interstrand crosslinks that inhibit DNA synthesis; this occurs in the S phase. B: Taxanes bind to microtubules and, by enhancing their stability and preventing disassembly, adversely affect their function. Taxanes act as mitotic inhibitors, blocking cells in the G2/M phase of the cycle and, if the concentration is sufficient, killing them in this phase.
▪ CLASSES OF AGENTS AND THEIR MODE OF ACTION
Many of the classical chemotherapeutic agents fall into one of three classes: alkylating agents, antibiotics, or antimetabolites. However, many of the newer and most widely used agents do not fall into any of these classes. This includes the platinum compounds, procarbazine, the vinca alkaloids, the taxanes, and the newest of all, the topoisomerase inhibitors and “targeted therapy” agents that target a specific pathway that may be elevated or vulnerable in some tumor cells.
An attempt to summarize the classification of chemotherapeutic drugs is presented in Table 27.1. A few of the most commonly used agents are described briefly, with emphasis on their characteristics and mechanism of action and comments on the extent to which they interact with radiation. A thorough discussion of their clinical usefulness is outside the scope of this book.
The effectiveness of at least some chemotherapeutic agents is dependent on the presence or absence of molecular oxygen, in much the same way as x-rays. This is not surprising, at least for drugs whose action is mediated by free radicals.
Alkylating Agents
The alkylating agents are highly reactive compounds with the ability to substitute alkyl groups for hydrogen atoms of certain organic compounds, including DNA. There are five classes of alkylating agents:
Nitrogen mustard derivatives, such as cyclophosphamide, chlorambucil, and melphalan.
Ethylenimine derivatives, such as thiotepa.
Alkyl sulfonates, such as busulfan.
Triazine derivatives, such as dacarbazine.
Nitrosoureas, including bischloroethylnitrosourea (BCNU) (carmustine), chloroethyl-cyclohexyl-nitrosourea (CCNU) (lomustine), and methyl CCNU.
Most of these drugs contain more than one alkylating group and therefore are considered polyfunctional alkylating agents. The nitrosoureas and dacarbazine have mechanisms and cytotoxicity over and above their ability to alkylate nucleic acids. As a class, alkylating agents are considered cell cycle nonspecific.
Nitrogen mustard is the prototype for three other useful alkylating agents: cyclophosphamide, chlorambucil, and melphalan. Nitrogen mustard given intravenously interacts rapidly with cells in vivo, producing its primary effect in seconds or minutes. By contrast, cyclophosphamide (Cytoxan) is inert until it undergoes biotransformation in the liver. Disappearance of injected cyclophosphamide from the plasma is biexponential, with an average half-life of 4 to 6.5 hours. Like all useful alkylating agents, cyclophosphamide produces toxicity in rapidly proliferating normal tissues. Chlorambucil (Leukeran) is an aromatic derivative of nitrogen mustard and is the slowest acting alkylating agent in general use. Melphalan (Alkeran, L-PAM) is a phenylalanine derivative of nitrogen mustard.
TABLE 27.1 Chemotherapeutic Agents
Compound Class Chemotherapeutic Agent
Diseases for which Drugs Are Useful (Indications)
Unique/Major Toxicity
Targeted Pathway/Receptor (Mechanism of Action)
Synergy with Radiation
Alkylating agents
Regular-dose therapy in chronic myelogenous leukemia (CML) (FDA approved) and polycythemia vera. High-dose therapy in bone-marrow transplant.
Myelosuppression pulmonary toxicity especially with total body irradiation (TBI) when used in high doses for bone marrow transplant.
DNA alkylation (i.e., interstrand crosslinks).
Busulfan (Myleran)—BSF
Carboplatin (Paraplatin)—Carbo, CBDCA
FDA approved for ovarian cancer, and used extensively in testicular cancer; squamous cell cancers of the head, neck, and cervix; and lung cancer.
Myelosuppression, especially thrombocytopenia, is dose limiting.
Produces intrastrand and interstrand crosslinks in DNA via association bonds with the platinum molecule, leading to DNA strand breakage during replication.
Carmustine (BiCNU)—BCNU, Bischloronitrosourea
FDA approved for brain tumors, multiple myeloma, Hodgkin disease, and lymphoma.
Myelosuppression, especially thrombocytopenia, which is slow in onset and cumulative, is dose limiting. Interstitial lung disease, including fibrosis, is rare but can occur with any dose. Weak synergy with radiation therapy (RT).
FDA approved for chronic lymphocytic leukemia (CLL) and low-grade lymphomas. Also used for Waldenström macroglobulinemia, multiple myeloma, hairy cell leukemia, and rarely in some solid tumors.
Myelosuppression is dose limiting and universal, and it can be cumulative.
FDA approved for many malignancies and used for even more. Most commonly used for breast carcinoma, non-Hodgkin lymphoma, ovarian carcinoma, and testicular cancer.
Myelosuppression is dose limiting, with leukopenia being most significant. Hemorrhagic cystitis common with doses more than 2 g/m2.
Cell cycle non-specific crosslinking Prodrug activated in liver.
FDA approved for the treatment of recurrent germ cell tumors. Used for many other tumor types, including adult sarcomas, lymphoma, Hodgkin’s disease, breast cancer, and ovarian cancer.
Myelosuppression, hemorrhagic cystitis, and central nervous system (CNS) toxicity are all fairly common and can be dose limiting. Hemorrhagic cystitis can largely be prevented by coadministration of the uroprotective agent mesna.
Non-specific cell cycle alkylating agent
Lomustine (CeeNU)—CCNU
FDA approved for primary brain tumors and Hodgkin disease. Also used in melanoma, multiple myeloma, other lymphomas, and breast cancer.
Myelosuppression, especially thrombocytopenia, is dose limiting and tends to be cumulative. Pulmonary fibrosis can occur with long-term administration. Weak synergy with RT.
FDA approved for various hematologic malignancies and solid tumors, but generally used less in the last decade. Still used for Hodgkin disease and topically for cutaneous T-cell lymphoma.
This drug is a powerful vesicant, so optimal extravasation precautions and rapid infusion are a must. Myelosuppression is expected and also often dose limiting. Secondary leukemia.
Used primarily for multiple myeloma, but also FDA approved for ovarian carcinoma. Could also be useful in high-dose chemotherapy/transplant settings and in regional perfusion of extremities for melanoma and sarcoma.
Myelosuppression is expected and is dose limiting. Recovery can be prolonged, and effects can be cumulative. Secondary leukemia.
Cell cycle non-specific alkylating agent.
Oxaliplatin (Eloxatin)
FDA approved for metastatic colorectal cancer in combination with 5-fluorouracil/leucovorin. It has been used as a single agent in this disease and is being studied in other malignancies.
Neurotoxicity, in the form of a transient neuropathy with each dose and a persistent cumulative typical sensory polyneuropathy, is very common and dose limiting.
Cell cycle non-specific intrastrand and interstrand crosslinks with two strong platinum association bonds in the molecule.
Procarbazine (Matulane)—N-methylhydrazine
FDA approved for Hodgkin disease and might also be useful in non-Hodgkin lymphoma, multiple myeloma, brain tumors, melanoma, and lung cancer.
Myelosuppression is expected and dose limiting, but anemia is uncommon. Hives and photosensitivity sometimes occur. Dietary restrictions.
Used for almost every class of solid tumor and lymphoma. FDA approved for testicular and ovarian cancers and transitional cell carcinoma.
Nephrotoxicity is dose limiting for an individual dose, whereas neurotoxicity, especially painful peripheral neuropathy, is dose limiting for cumulative doses. Cumulative ototoxicity is also common. Intermediate synergy with RT.
Produces intrastrand and interstrand crosslinks in DNA via association bonds with the platinum molecule, leading to DNA strand breakage during replication.
Cisplatin (Platinol)—cDDP, DDP, Cis-platinum, Cis-diammine-dichloroplatinum (II)
Antibiotics
FDA approved for germ cell tumors, Hodgkin disease, and squamous cell cancers. Used off-label for melanoma, ovarian cancer, and Kaposi sarcoma. Also used as a sclerosing agent for malignant pleural or pericardial effusions.
Pulmonary toxicity, including reversible and irreversible fibrosis, is dose limiting. Strong synergy with RT.
Causes DNA strand breaks directly in normal and neoplastic cells.
FDA approved for Wilms tumor, Ewing sarcoma, rhabdomyosarcoma, uterine carcinoma, germ cell tumors, and sarcoma botryoides, and also used for other sarcomas, melanoma, acute myeloid leukemia, ovarian cancer, and trophoblastic neoplasms.
This drug is a moderate vesicant. Myelosuppression is dose limiting. Nausea, vomiting, skin erythema, acneiform lesions, and hyperpigmentation are common. Strong synergy with RT.
Inhibits transcription by complexing with DNA and prevents elongation by RNA polymerase
FDA approved for various cancers and used for many more. Most commonly used for breast carcinoma, adult sarcomas, pediatric solid tumors, Hodgkin disease, non-Hodgkin lymphomas, and ovarian cancer.
Doxorubicin is a potent vesicant, and extravasation precautions are a must. Myelosuppression is universal and usually dose limiting with each individual cycle. Cardiotoxicity is common and can be dose limiting, although usually subclinical. Chronic, cumulative cardiomyopathy is expected when total dose exceeds 400-500 mg/m2. Strong synergy with RT. Recall skin reactions that correspond to prior RT treatment fields may develop, and can be severe. Concurrent RT or initiation of RT within 2 weeks of administration of doxorubicin should be avoided.
FDA approved for adenocarcinomas of the stomach and pancreas. Also used commonly in breast cancer and lung cancer.
Mitomycin C is a vesicant; extravasation precautions are a must. Myelosuppression is expected and is dose limiting, with a white blood cell nadir at 4 weeks and full recovery at 6-7 weeks. Strong synergy with RT.
FDA approved for colon, rectum, gastric, pancreas, and breast carcinomas and used for a wide range of other neoplasms in combination regimens. Used for intrahepatic arterial infusion for liver metastases from gastrointestinal (GI) tumors and also used topically for various cutaneous neoplasms and disorders.
GI toxicities, primarily mucositis for bolus injection and diarrhea for prolonged infusions, are dose limiting. Rare patients with dihydropyrimidine dehydrogenase deficiency have excessive GI toxicity. Dermatitis and other cutaneous toxicities, Mincluding hand-foot syndrome, are common. Intermediate synergy with RT.
Inhibitor of thymidylate synthase; partially cell cycle dependent.
FDA approved for metastatic breast cancer and metastatic colorectal cancer. Used also in head and neck squamous cell cancer.
Myelosuppression and palmar-plantar erythrodysesthesia are dose limiting. Diarrhea, fatigue, stomatitis, and hyperbilirubinemia are uncommon. Intermediate synergy with RT.
Acute myelogenous leukemia (AML), acute lymphoblastic lymphoma (ALL), and non-Hodgkin lymphoma. Intrathecal use in acute leukemia.
Myelosuppression, often severe and prolonged, is dose limiting. Neurologic toxicity, mostly central with ataxia being predominant, is common and usually mild, but it is dose dependent and could leave permanent dysfunction. It is more common with intrathecal administration.
Incorporated into DNA during replication, leading to strand termination; S phase specific. Penetrates blood-brain barrier.
Fludarabine (Fludara)—FAMP
FDA approved for the treatment of CLL. Also used for low-grade lymphomas and for AML.
Neurotoxicity, including cortical blindness, confusion, somnolence, coma, and demyelinating lesions, is dose limiting, but the lower doses conventionally used rarely produce these side effects.
Purine analog. Inhibits DNA polymerase. Only Partially cell cycle specific.
Gemcitabine (Gemzar)
FDA approved for advanced pancreatic adenocarcinoma, non-small cell lung cancer (NSCLC), and metastatic breast cancer; extensively used in bladder cancer also.
Myelosuppression, including anemia, is mild but dose limiting. Strong synergy with RT even at low doses of drug.
A nucleoside analogue that exhibits S-phase-specific cytotoxicity. Inhibits DNA synthesis.
FDA approved for CML; commonly used for other myeloproliferative disorders and also used occasionally for metastatic melanoma, refractory ovarian carcinoma, and squamous cell carcinoma of the cervix and head and neck.
Myelosuppression is common and dose limiting. Other toxicities include rash, headache, fever, and hyperuricemia. Nausea and vomiting are uncommon. Liver toxicity and serious neurologic toxicity are rare. Weak synergy with RT.
Inhibitor of ribonucleotide reductase, which converts nucleotides to the deoxyribose forms for DNA synthesis; cell cycle dependent. Penetrates blood-brain barrier.
FDA approved for a wide spectrum of malignant and nonmalignant diseases. Most often used for acute leukemias, lymphomas, breast cancer, bladder cancer, squamous cell cancers, and sarcomas.
Myelosuppression is expected and is usually dose limiting. Renal toxicity is uncommon and usually reversible, but can be severe. Encephalopathy is rare with moderate to low-dose therapy but is more common with high doses, intrathecal administration, or concomitant CNS radiation. It can be severe and permanent. Drug should be administered prior to rather than concurrently or following brain RT when feasible to lessen risk of leukoencephalopathy. Weak synergy with RT.
Interferes with nucleotide synthesis by inhibiting dihydrofolate reductase; cell cycle dependent. Penetrates blood-brain barrier at high intravenous doses.
FDA approved for various malignant and nonmalignant conditions. Used in oncology for lymphoid malignancies, for palliative care, and for management of side effects/toxicities.
Toxicity is mostly in the form of constitutional symptoms, including mood changes (depressive, anxious, or euphoric), insomnia, indigestion, enhanced appetite, weight gain, acne, and cushingoid features. Other side effects may be more serious but are less common. Hyperglycemia and increased stomach acid predisposing to ulceration occur acutely, whereas osteopenia, cataracts, skin atrophy, and adrenal insufficiency occur with prolonged use.
Same as naturally occuring ones.
Prednisone (Deltasone, others)
Enzymes
FDA approved for ALL; also used in AML, late-stage CML, CLL, and non-Hodgkin lymphomas.
Hypersensitivity can be life threatening, requiring anaphylaxis precautions and a 2-unit test dose. Coagulopathy is common and requires monitoring. Lethargy, somnolence, fatigue, depression, and confusion are seen, as are pancreatitis and fever.
Catalyzes the hydrolysis of amino acid asparagine, which is an essential amino acid required by rapidly proliferating cells, to aspartic acid.
I-Asparaginase (Elspar)—Colaspase
Steroidal progestational agents
FDA approved for treatment of breast and endometrial carcinoma. Also used for renal cell carcinoma and for appetite stimulation in HIV disease and cancer patients.
Toxicities are similar to those of other progestins as noted previously. They include menstrual changes, hot flashes, edema, weight gain, fatigue, acne, hirsutism, anxiety, depression, sleep disturbance, and headache. Urinary frequency can also occur. Nausea, vomiting, diarrhea, skin rash or allergy, jaundice, and thrombophlebitis are uncommon.
Little known about drug targets.
Megestrol acetate (Megace)—Megestrol
Targeted therapy
FDA approved for combination with 5-FU for first- and second-line treatment of metastatic colorectal cancer; for combination with carboplatin and paclitaxel; for unresectable, locally advanced, recurrent, or metastatic non-squamous, non-small cell lung cancer; and for combination with interferon alpha for metastatic renal cell cancer.
Most toxicities related to inhibition of angiogenesis. GI perforation is the major life-threatening side effect. Treatment can also inhibit wound healing and may prevent surgical incisions to close, also leading to fatality in some instances. Bleeding in stomach, brain, nose, and vagina. Common side effects are nosebleeds, high blood pressure, headache, and inflammation.
Inhibits the function of vascular endothelial growth factor. Causes regression of existing tumor vessels. Makes existing tumor vessels more functional in supplying oxygen and chemotherapy. Inhibits new tumor vessel growth.
Colorectal cancer, lung cancer, head and neck cancer.
Self-limiting sterile, nonsup-purative acne-like skin rash is common. Resolves with cessation of drug. Patients exhibiting a grade 2 rash or above have better survival. Strong synergy with RT.
Blocks EGFR receptor dimerization and tyrosine kinase phosphorylation, which inhibits tyrosine kinase pathway signal transduction.
FDA approved for treatment of CML in the frontline setting, in accelerated phase, and in blast crisis. It is also approved for treatment of recurrent inoperable or metastatic gastrointestinal stromal tumors.
There is no definite dose-limiting toxicity of imatinib. Myelosuppression is significant in CML but mild in gastrointestinal stromal tumors. Hepatotoxicity is common but usually mild. Liver function tests should be monitored closely during therapy. Fluid retention is common but usually mild, as are nausea, vomiting, and diarrhea. Rash and fever are uncommon.
Specific receptor tyrosine kinase inhibitor, which selectively inhibits the tyrosine kinases of the bcr-abl, c-kit, and platelet-derived growth factor (PDGF) receptors.
Soon to be FDA approved for BRCA-mutation-positive breast, ovarian, and prostate cancer. Doubling of progression-free survival for patients with triple negative breast cancer when inhibitors are combined with gemcitabine and carboplatin.
Dizziness, nausea, vomiting, diarrhea, lymphopenia, anemia, and fatigue.
PARP inhibitors block DNA base excision, leading to the collapse of replication forks and generation of DNA double-strand breaks. Cells possessing BRCA mutations cannot repair PARP inhibitor-induced DNA double-strand breaks by homologous recombination.
FDA approved for relapsed or refractory low-grade or follicular, CD20-positive, B-cell lymphomas.
Fever, chills, and malaise are common during administration, even with premedication with acetaminophen and diphenhydramine. Other infusion-related symptoms include nausea, vomiting, flushing, urticaria, angioedema, hypotension, dyspnea, bronchospasm, fatigue, headache, rhinitis, and pain at disease sites. These symptoms are generally self-limited, improve with slowing of the infusion, and resolve after infusion. Short-lived myelosuppression, abdominal pain, and myalgia are uncommon. Arrhythmias and angina pectoris are rare.
Directed against the B-cell surface antigen CD20.
Trastuzumab (Herceptin)
FDA approved for HER2/neu overexpressing metastatic or locally advanced breast cancer; has shown clinical benefit as a single agent and in conjunction with paclitaxel-based chemotherapy.
Common toxicities include acute fever, chills, nausea, vomiting, and headache. Trastuzumab seems to worsen leukopenia, anemia, and diarrhea when given with chemotherapy compared with chemotherapy alone. Also, trastuzumab could have uncommon acute cardiotoxicity, which might add to the more common anthracycline-induced cardiotoxicity; therefore, the use of trastuzumab with doxorubicin is not indicated by the FDA.
Directed against the HER2/neu growth factor receptor overexpressed on many invasive breast carcinomas; mechanism of action for clinical activity in breast cancer is unknown, but could be comple-ment-mediated cell lysis, antibody-dependent cellular cytotoxicity, or induction of apoptosis.
Taxanes
FDA approved for metastatic breast cancer and first- and second-line NSCLC. Clinical experience increasing in ovarian cancer and other epithelial neoplasms.
Myelosuppression is universal and dose limiting. Alopecia is also universal. Edema and fluid accumulation, including pleural effusions and ascites, are common and can be dose limiting. Fluid accumulation is partially preventable with corticosteroid treatment before and after each cycle of docetaxel. Mild sensory or sensorimotor neuropathy is common.
Inhibits the mitotic spindle apparatus by stabilizing tubulin polymers, leading to death of mitotic cells.
Docetaxel (Taxotere)
Paclitaxel (Taxol, Onxol)
FDA approved for salvage therapy in ovarian cancer and for breast cancer in both the metastatic and adjuvant setting. Used also in lung cancer, head and neck cancers, and bladder cancer.
Paclitaxel is an irritant or mild vesicant when extravasated into subcutaneous tissue. Myelosuppression, predomi-nantly neutropenia, is expected and is dose limiting. Shorter infusions of the same dose produce less neutropenia. Mucositis is with very common, particularly with longer infusions. Peripheral neuropathy is common, usually mild, and increases with cumulative dose. Acute neuromyopathy is also common and occurs for several days after each dose. Hypersensitivity reactions to paclitaxel, including urticaria, wheezing, chest pain, dyspnea, and hypotension, are common but are reduced in frequency and severity by premedication with corticosteroids and H1 and H2 histamine receptor blockers (recommended regimen is dexamethasone 20 mg PO 12 and 6 hours prior to paclitaxel and diphenhydramine 50 mg and cimetidine 300 mg IV 30 minutes prior to paclitaxel). Weak synergy with RT.
Inhibits depolymerization of tubulin in the spindle apparatus, thereby inducing apoptosis in dividing cells.
FDA approved for germ cell tumors and small cell lung cancer (SCLC). Also used for lymphomas, AML, brain tumors, NSCLC, and as high-dose therapy in the transplant setting for breast cancer, ovarian cancer, and lymphomas.
Myelosuppression, primarily leukopenia, is universal and dose limiting. Nausea and vomiting are common with PO administration but rare when the drug is given IV. Stomatitis and diarrhea are rare with normal doses but common with high doses. Secondary AML has been reported after etoposide.
Partially cell cycle specific. Topoisomerase II inhibitor.
Etoposide (Vespid)—VP-16, Epipodophyllotoxin; also available as Etoposide Phosphate (Etopophos)
Irinotecan (Camptosar)—CPT-11
Irinotecan is FDA approved for refractory or recurrent metastatic colon cancer, and it has now been used in other malignancies, including lung cancer, ovarian cancer, and lymphoma.
Myelosuppression, primarily neutropenia, is common and dose limiting. Diarrhea is also common and can be dose limiting.
Partly cell cycle specific. Topoisomerase I inhibitor.
Vinca alkaloids
FDA approved for multiple hematologic and solid neoplasms. Most often used for Hodgkin disease, non-Hodgkin lymphoma, germ cell tumors, and breast cancer.
Vinblastine is a soft tissue vesicant, requiring extravasation precautions during administration. Myelosuppression, especially leukopenia, is expected and dose limiting.
Inhibitor of tubulin polymerization and thereby mitosis; G2 phase specific
FDA approved for Hodgkin disease and other lymphomas, acute leukemias, rhabdomyosarcoma, neuroblastoma, and Wilms tumor. Used for many other neoplasms as well.
Vincristine is a vesicant and should be administered with extravasation precautions. Neurotoxicity is dose limiting in the form of peripheral neuropathy, which is related to total cumulative dose.
Inhibitor of tubulin polymerization and thereby mitosis; G2 phase specific.
FDA approved for the treatment of relapsed metastatic breast cancer and for NSCLC as a single agent or combined with a platinating agent.
Vinorelbine is a mild vesicant, requiring exravasation precautions. Myelosuppression, mostly leukopenia, is expected and dose limiting. Neurotoxicity in the form of neuropathy is less common and milder than that seen with vincristine. Tumor pain during administration has been reported.
Inhibitor of tubulin polymerization and thereby mitosis; G2 phase specific.
Luteinizing hormone-release hormone (LHRH)
FDA approved for advanced prostate cancer and used also in metastatic breast cancer.
Toxicity is mild. Endocrine side effects are most prominent and include hot flashes, diminished libido, impotence, gynecomastia, amenorrhea, and breakthrough vaginal bleeding.
Inhibits pituitary-gonadal axis function; causes steroid hormone withdrawal from dependent tissues, including prostate cancer and breast cancer cells.
Goserelin acetate (Zoladex)
Only gold members can continue reading. Log In or Register to continue