Additionally, patients are not exposed to the potentially harmful effects of ionizing radiation.
TABLE 12.1 Practical Evaluation of Pediatric Chest Wall Lesions | ||
|---|---|---|
|

TABLE 12.2 Advantages and Disadvantages of Imaging Modalities for Evaluation of Pediatric Chest Wall Lesions | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
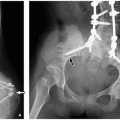
 FIGURE 12.1 Oblique rib radiograph with a radiopaque marker placed in area of palpable mass. |
TABLE 12-3 CT Protocol for Chest Wall Lesions | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
and postcontrast T1-weighted FS sequence provide information about the vascularity of soft tissue masses and vascular anomalies.
 FIGURE 12.2 Skeletal chest wall anatomy. |
Ossification of the skeletal elements begins in utero and continues until the 25th year of life. Due to differences in muscle mass and ossification, the chest wall of infants and children is more elastic and compliant than in adults. This results in lower resting lung volumes and a less efficient respiratory mechanism that predisposes infants and young children to atelectasis. The osseous and soft tissue components gradually become stiffer with age.16
 FIGURE 12.3 Layers of the chest wall. |
 FIGURE 12.4 Chest wall layers as seen on axial CT image. |
TABLE 12.4 Key Features of Common Primary Pediatric Chest Wall Lesions | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
sequences may negate the need for ionizing radiation in preoperative evaluation32 (Fig. 12.6).
 FIGURE 12.5 Pectus excavatum in a 10-year-old boy. PA (left) and lateral (right) radiographs of the chest demonstrate posterior depression (arrow) of the sternum with a narrowed anteroposterior diameter of the thorax and leftward shifting of the mediastinal structures. |
 FIGURE 12.6 Pectus excavatum in a 16-year-old boy with chest asymmetry. Axial 2D balanced gradient-echo T2-weighted fat-saturated MR image demonstrates rightward tilt and depression of the lower sternum with compression of the right atrium (asterisk). The heart is slightly deviated to the left. Haller index is 3.7 (272.4/74.1). |
anterior chest wall “mass”19 (Fig. 12.8). When the etiology is not evident on physical exam, chest radiographs with a BB marker placed at the area of concern are usually sufficient. US may also provide adequate evaluation, especially for cartilaginous lesions. If CT is performed, 3D reformatted images are useful to clearly depict the prominent contour. Management is reassurance.
 FIGURE 12.7 Pectus carinatum in a 10-year-old boy with neurofibromatosis type 1 and prior spinal fixation for scoliosis. Sagittal CT image shows anterior protrusion of the sternum (arrow) resulting in increased anteroposterior diameter of the chest. |
 FIGURE 12.8 Prominent convexity in a 6-month-old boy with a chest wall “mass.” Axial CT image shows asymmetric prominence of the right anterior seventh costal cartilage (arrow), which accounted for the palpable abnormality. |
 FIGURE 12.9 Rib fusion in a 4-year-old boy. Chest radiograph shows complex scoliosis with multiple thoracic vertebral anomalies and bilateral posterior rib fusions (asterisks). |
 FIGURE 12.10 Bifid rib in a 2-year-old boy referred for a chest mass. Three-dimensional reformatted CT image shows the right third bifid rib (arrow), which accounted for the palpable mass. |
 FIGURE 12.11 Intrathoracic rib in a 3-year-old boy. Oblique radiograph of the ribs shows a vertically oriented osseous structure (arrow) coursing from the right posterior fifth costovertebral junction to the posterior sixth rib. |
 FIGURE 12.12 Cervical ribs in a 2-year-old girl with prior sternotomy for truncus arteriosus repair. Coned chest radiograph shows bilateral cervical ribs (arrows) articulating with the transverse processes of C7. |
 FIGURE 12.13 Cleidocranial dysostosis in a 3-year-old boy. A: Chest radiograph shows absent bilateral clavicles. B: Lateral skull radiograph shows open skull sutures, large fontanelles, multiple wormian bones, and underdeveloped paranasal sinuses. |
 FIGURE 12.14 Poland syndrome in a 15-year-old girl with chest deformity. A: Frontal chest radiograph demonstrates diffuse lucency of the right hemithorax. B: Axial enhanced CT image shows absent pectoralis muscles and severely diminished breast tissue on the right. |
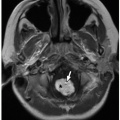
Radiographs and CT may show focal osteopenia, cortical irregularity, periosteal reaction, and contiguous soft tissue swelling. Findings are apparent on radiographs only after 7 to 10 days. Cortical irregularity and fluid adjacent to the bone and within the joint can be seen with US. Associated soft tissue changes on US include increased subcutaneous echogenicity, loss of normal soft tissue architecture, and reticular anechoic subcutaneous edema.54,55 US can be used to identify and guide drainage of superficial abscesses, which appear as hypoechoic or anechoic collections with posterior acoustic enhancement and peripheral hyperemia. Deep infection is better evaluated with CT or MRI. Although CT is superior at demonstrating osseous erosion, MRI best depicts the early changes of osteomyelitis. Abnormal marrow edema is evidenced by high T2-weighted and low T1-weighted signal intensity. Intravenous contrast may clarify regions of abscess formation (Fig. 12.15). Bone scintigraphy is sensitive for early detection but lacks anatomic detail.
TABLE 12.5 Differential Diagnosis of Aggressive-Appearing Pediatric Chest Wall Lesions | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 FIGURE 12.15 Staphylococcus aureus abscess and osteomyelitis in a 10-year-old boy with leukemia and disseminated infection. Axial T2-weighted MR image (top left), T1-weighted postcontrast fat-saturated MR image (bottom left), diffusion-weighted MR image (top right), and fused PET-MR image (bottom right) show a focal collection (arrows) with high T2 signal, peripheral enhancement, restricted diffusion, and hypermetabolic activity at the left anterior sixth costochondral junction with abnormal signal in the adjacent rib and soft tissues. A smaller collection is present on the right. Abnormal marrow signal in the spine was related to leukemic involvement. |
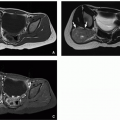
 FIGURE 12.16 Pulmonary tuberculosis with sternal osteomyelitis and abscess in a 15-year-old boy. Axial enhanced lung window CT image (top) shows nodular and tree-in-bud pattern opacities with areas of cavitation. Axial enhanced soft tissue window CT image (middle) shows partially calcified subcarinal lymph nodes (arrow) and sternal destruction with surrounding soft tissue thickening and fluid collections. Sagittal bone window CT image (bottom) more clearly demonstrates the sternal osteolysis with adjacent sclerosis and cortical thickening. |
 FIGURE 12.17 Empyema necessitates in a 1-year-old girl with a history of gastropleural fistula and empyema. Coronal enhanced soft tissue window CT image shows a left pleural collection with surrounding pleural thickening and enhancement. The collection extends laterally through the eighth intercostal space into the subcutaneous tissues of the left lateral chest wall. There is significant atelectasis of the left lung. Pleural fluid culture showed multimicrobial infection. |
 FIGURE 12.18 Lipoma in a 13-year-old girl. This 4 cm lesion resected from the chest subcutis consists grossly of pale yellow lobulated adipose tissue (left). Microscopically, the adipose tissue is traversed by thin septa containing mature fibroblasts (right, hematoxylin and eosin, original magnification, 100×). |
 FIGURE 12.19 Lipoma in a 4-year-old boy who presented with right sided chest discomfort. Coronal enhanced CT image shows a well-defined, homogeneous fat attenuation mass (arrow) along the right lateral chest that extending into the fourth and fifth intercostal space. |
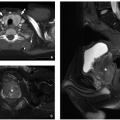
density mass. CT and MRI appearance is heterogeneous with fatty and nonfatty elements and occasionally a combination of nonenhancing cystic areas and enhancing soft tissue66 (Fig. 12.21).
 FIGURE 12.20 Lipoblastoma in a 5-year-old boy. There was longstanding diffuse involvement (lipoblastomatosis) of the chest wall, axilla, and brachial plexus. Here, the features are of a “mature” lipoblastoma with adipose tissue, prominent fibrous septa, and only rare lipoblasts (hematoxylin and eosin, original magnification, 200x). |
 FIGURE 12.21 Lipoblastoma in a 12-year-old girl who presented with posterior chest wall deformity. Axial enhanced CT image (top), T1-weighted MR image (middle), and T1-weighted fat-saturated MR image (bottom) demonstrate a predominantly fatty lesion insinuating throughout paraspinal musculature, axilla, and intercostal regions bilaterally. |
involvement, which is most common in the lungs, gastrointestinal tract, and heart.68,72,73 Grossly, myofibroma/myofibromatosis is a firm white mass and variably well circumscribed. Microscopically, whorled bundles of fibroblastic cells are seen. A characteristic feature is the involvement of vessel walls (Fig. 12.24).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


