Abstract
Chest wall lesions may arise in the subcutaneous soft tissues or the thoracic cage, which includes the ribs and associated muscle, vessels, and nerves. Evaluation of the subcutaneous soft tissues on the chest x-ray is limited to contour irregularities and often requires CT or MRI. Thoracic cage abnormalities are most often accurately appreciated on the chest x-ray when the ribs are involved. Chest wall tumors include primary benign and malignant bone tumors, hematologic tumors, metastases, and invasion from lung tumors. Infections that may spread from the lung through the pleura and chest wall include tuberculous and fungal or bacterial empyema. Rib fractures with hematomas are usually confirmed by the history.
Keywords
actinomycosis, blastomycosis, empyema necessitans, metastases, multiple myeloma, neurofibroma, nocardiosis, Pancoast tumor, primary benign and malignant bone tumors, schwannoma, tuberculosis
Questions
- 1.
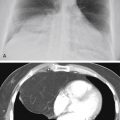
The most likely diagnosis in the afebrile patient in Fig. 2.1 is:
- a.
Neurofibroma.
- b.
Lipoma.
- c.
Multiple myeloma.
- d.
Osteosarcoma.
- e.
Chondrosarcoma.

Fig. 2.1
- a.
- 2.
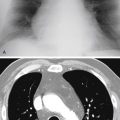
The most likely diagnosis in Fig. 2.2 is:
- a.
Ewing sarcoma.
- b.
Osteosarcoma.
- c.
Chondrosarcoma.
- d.
Metastatic lung cancer.
- e.
Plasmacytoma.

Fig. 2.2
- a.
Mark the following questions True or False:
- 3.
_____ Chest wall lesions may sometimes be distinguished from pulmonary nodules by identification of an incomplete border.
- 4.
_____ Lipoma is a common chest wall lesion.
- 5.
Neurofibroma of an intercostal nerve will probably cause rib destruction.
- 6.
_____ Rib detail views or computed tomography (CT) scans are rarely needed to identify the rib destruction of a primary bone tumor in the chest wall.
- 7.
_____ Metastases and multiple myeloma are among the most common causes of a chest wall mass with associated rib destruction in an adult.
- 8.
_____ Ewing tumor and neuroblastoma should be considered when a chest wall mass is observed in a child or young adult.
Discussion
Chest wall lesions ( Chart 2.1 ) may arise from both extrathoracic and intrathoracic locations as well as normal and abnormal structures. Common extrathoracic causes of radiographically visible opacities include nipples, moles, and various cutaneous lesions (e.g., neurofibromas of von Recklinghausen disease). 155 , 535 Extrathoracic chest wall opacities are seen as soft-tissue opacities with an incomplete, sharp border ( Fig. 2.3 ). The border is produced by the interface of the mass with air and is lost where the mass is continuous with the soft tissues of the chest wall. Cutaneous lesions should not have the tapered borders that are seen in Fig. 2.1 . The tapered border indicates displacement of the pleura inward by the mass and has been described as an extrapleural sign. 151 Physical examination is also essential in the evaluation of cutaneous lesions. Nipple shadows may be easily identified when they are symmetric and when their borders are incomplete, but caution is warranted. 387 Repeat examination with small, lead nipple markers should be performed if there is any possibility of confusing a nipple shadow with a pulmonary nodule.
- I.
Nipples, 387 supernumerary nipples 206
- II.
Artifact
- III.
Skin lesions (e.g., moles, neurofibromas, extrathoracic musculature) 88
- IV.
Mesenchymal tumors (muscle tumors, fibromas, lipomas, 137 liposarcoma, 63 desmoid tumor, 109 synovial sarcoma 191 )
- V.
Neural tumors (schwannoma, 459 neurofibroma, ganglioneuroma, neuroblastoma 580 )
- VI.
Hodgkin and non-Hodgkin lymphoma 438
- VII.
Vascular tumors (angiosarcoma, glomus tumor, hemangioma, Kaposi sarcoma) 63 , 352 , 579 , 580
- VIII.
Benign bone tumors (fibrous dysplasia, osteochondroma, giant cell tumor, aneurysmal bone cyst, fibroma, chondromyxoid fibroma) 579
- IX.
Malignant bone tumors (metastases, 325 multiple myeloma, plasmacytoma [solitary myeloma]) 580
- X.
Ewing sarcoma, chondrosarcoma, 419 osteosarcoma, 191 fibrosarcoma, malignant undifferentiated pleomorphic sarcoma
- XI.
Hematoma
- XII.
Rib fractures
- XIII.
Infection (actinomycosis, 618 aspergillosis, 14 nocardiosis, blastomycosis, tuberculosis, empyema necessitans, osteomyelitis [rare]) 210
- XIV.
Thoracopulmonary small cell (Askin) tumor 157
- XV.
Invasion by contiguous mass (lung cancer) 167 , 313
- XVI.
Lymphangioma (cystic hygroma)

Intrathoracic chest wall lesions are radiologically visible because of their interface with aerated lung. Like the cutaneous lesions, their borders are incomplete where they are contiguous with the chest wall. 132 Thus the incomplete border is helpful in distinguishing chest wall lesions from pulmonary lesions (answer to question 3 is True ), but not in distinguishing cutaneous from intrathoracic chest wall lesions. The tapered superior and inferior borders, however, are valuable signs for confirming an intrathoracic extrapulmonary location. Unfortunately, the tapered border may not be observed if the lesion is seen en face ; in fact, the lesion may not be visible. Lateral and oblique cone-down views are frequently helpful in eliciting this sign.
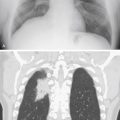
Lipomas are common chest wall lesions 313 and may be seen as either subcutaneous or intrathoracic masses ( Fig. 2.4, A ). (Answer to question 4 is True .) They may even grow between the ribs, presenting as both intrathoracic and subcutaneous masses. Physical examination reveals a soft, movable mass when there is a significant subcutaneous component. CT should show the extent of the mass and, more importantly, confirm that the lesion is of fat attenuation 137 ( Fig. 2.4, B ).