As in the brain, the sensitivity of diffusion-weighted imaging (DWI) to ischemic damage in the spinal cord may provide early identification of infarction. Diffusion anisotropy may enhance the detection and understanding of damage to the long fiber tracts with clinical implications for diseases such as multiple sclerosis and amyotrophic lateral sclerosis and may also yield insight into damage that occurs with spondylotic and traumatic myelopathy. This article reviews the basis for DWI for the evaluation of the spinal cord, osseous, and soft tissues of the spine and reviews the imaging appearance of a variety of disease states.
Key points
- •
Diffusion imaging is a powerful technique in widespread use in whole-body imaging that is a valuable adjunct to routine imaging protocols for the spine.
- •
Diffusion imaging adds sensitivity and specificity in evaluating the osseous and soft tissue structures of the spine for neoplastic involvement.
- •
Diffusion imaging adds sensitivity and specificity in evaluating the osseous and soft tissue structures of the spine in cases of suspected infection.
- •
Diffusion imaging can contribute valuable information to the evaluation of lesions of the spinal cord.
- •
Protocol optimization and pending technical advances can and will provide critical improvements in image quality, which should lead to routine use in the evaluation of diseases of the spine.
Introduction
The imaging assessment of the diffusion characteristics of water molecules on an intracellular and extracellular space level can herald powerful information about normal and abnormal tissues and processes. Diffusion-weighted imaging (DWI), a technique typically based on echo planar imaging (EPI), has been widely available for clinical purposes since the early 1990s. DWI rapidly achieved universal use for the evaluation of brain diseases, improving sensitivity and specificity of magnetic resonance (MR) imaging for a variety of disease states, including infarction, infection, inflammation, and hemorrhage. Of late, DWI has achieved greater importance in evaluation of the abdomen, pelvis, prostate, and breast with increasingly routine use in day-to-day practice. Although DWI should be equally sensitive to diseases of the spine, it has been used far less frequently in this region. This is mainly because of the challenges placed by the spine’s heterogeneous magnetic environment, the small size of the spinal cord, and motion in and around the spine.
There is, however, a range of current and potential applications for DWI in the spine. As in the brain, the sensitivity of DWI to ischemic damage in the spinal cord may provide early identification of infarction. Diffusion anisotropy may enhance the detection and understanding of damage to the long fiber tracts with clinical implications for diseases such as multiple sclerosis and amyotrophic lateral sclerosis. Diffusion anisotropy may also yield insight into damage that occurs with spondylotic and traumatic myelopathy. DWI has also been exploited for its ability to detect and characterize lesions of the spinal marrow and potentially differentiate between benign and malignant vertebral compression fractures. Although technical limitations persist to a varying degree, the applications for DWI in the spine have been extensively investigated. Despite challenges and lingering controversy over clinical utility for some applications, DWI is increasingly becoming part of the routine clinical spine MR imaging regimen. This article reviews the basis for DWI for the evaluation of the spinal cord, osseous, and soft tissues of the spine and reviews the imaging appearance of a variety of disease states.
Introduction
The imaging assessment of the diffusion characteristics of water molecules on an intracellular and extracellular space level can herald powerful information about normal and abnormal tissues and processes. Diffusion-weighted imaging (DWI), a technique typically based on echo planar imaging (EPI), has been widely available for clinical purposes since the early 1990s. DWI rapidly achieved universal use for the evaluation of brain diseases, improving sensitivity and specificity of magnetic resonance (MR) imaging for a variety of disease states, including infarction, infection, inflammation, and hemorrhage. Of late, DWI has achieved greater importance in evaluation of the abdomen, pelvis, prostate, and breast with increasingly routine use in day-to-day practice. Although DWI should be equally sensitive to diseases of the spine, it has been used far less frequently in this region. This is mainly because of the challenges placed by the spine’s heterogeneous magnetic environment, the small size of the spinal cord, and motion in and around the spine.
There is, however, a range of current and potential applications for DWI in the spine. As in the brain, the sensitivity of DWI to ischemic damage in the spinal cord may provide early identification of infarction. Diffusion anisotropy may enhance the detection and understanding of damage to the long fiber tracts with clinical implications for diseases such as multiple sclerosis and amyotrophic lateral sclerosis. Diffusion anisotropy may also yield insight into damage that occurs with spondylotic and traumatic myelopathy. DWI has also been exploited for its ability to detect and characterize lesions of the spinal marrow and potentially differentiate between benign and malignant vertebral compression fractures. Although technical limitations persist to a varying degree, the applications for DWI in the spine have been extensively investigated. Despite challenges and lingering controversy over clinical utility for some applications, DWI is increasingly becoming part of the routine clinical spine MR imaging regimen. This article reviews the basis for DWI for the evaluation of the spinal cord, osseous, and soft tissues of the spine and reviews the imaging appearance of a variety of disease states.
Diffusion-weighted MR imaging
DWI is a powerful tool for tissue investigation with MR imaging. By sensitizing the MR image to perturbations of the random motion of water molecules in tissues, DWI provides unique insight into pathologic physiology.
DWI revolutionized the evaluation of patients with suspected stroke by providing exquisite sensitivity to the presence of brain infarction, almost immediately after onset. DWI also provides the critical ability to differentiate chronic ischemic brain changes from those caused by recent stroke in patients who present in the subacute stroke setting. Perhaps the most impactful role of cranial DWI is in characterization of brain lesions—the differentiation of stroke and abscess from tumor and the assessment and surveillance of demyelinating disease. Of late, DWI has become popular for imaging outside the brain and is now commonly used in the routine MR imaging study of the breast, prostate, abdomen and pelvis, providing a boost in lesion detection. DWI also offers valuable characterization information useful in the differentiation of malignant from benign lesions as well as tumor from reactive and treatment-related changes.
Technical Considerations
Typically based on clinically available single-shot EPI scanning techniques, DWI is rapidly acquired and motion resistant. Although nearly ideal for imaging of the brain, EPI faces significant challenges in the spine. Bulk physiologic motion within the chest and abdomen or from swallowing and motion from the spinal cord itself are sources of artifact. Susceptibility variation associated with the osseous structures and field variations adjacent to the cervicothoracic junction and the lungs may cause severe distortion. The small size of the spinal cord and adjacent structures requires smaller voxel sizes and thus requires an inherently high signal-to-noise ratio (SNR) acquisition technique. As a result, application of DWI to the vertebral column and the spinal cord has been far less popular than elsewhere.
Alternative techniques based on single-shot and line scan fast spin echo ( Fig. 1 ) have been investigated but have failed to achieve clinical availability despite potential advantages over EPI. With minor modifications to current EPI-based protocol parameters, diagnostic quality studies of the spine can be obtained ( Fig. 2 ). Reduced B values (400–500) and minimized frequency encoding each reduces echo times (TE) leading to improved SNR and reduced distortion ( Box 1 ).
Repetition time (TR), echo time (TE) minimum
Frequency (General Electric): minimum (64 if possible), Siemens 192
Phase 192–256
Field of view 26
3–4 mm, skip 1
4 nex, acquisitions
B value – 500
Recent and continuing technical innovations greatly affect EPI DWI of the spine. Applying the 3 diffusion gradients simultaneously instead of sequentially (3 in 1, GE, Waukesha, WI) allows much shorter TE values, which boosts SNR, reduces distortion, and shortens scan times ( Fig. 3 ). Parallel imaging–capable spine coils allow DWI at reduced TE values, preserving SNR and reducing susceptibility effects ( Fig. 4 ). More powerful gradient systems also allow shorter TE values at a given B value, yielding either improved image quality or the use of higher B values. Recently available techniques such as multishot EPI ( Fig. 5 ) and restricted field-of-view (FOV) DWI ( Fig. 6 ) are practical and artifact resistant, promising better suitability to applications in body and spine. As the quality of the clinical diffusion image improves, DWI will gain even wider use in the routine diagnostic workup of spinal disorders.
Scientific study of diffusion imaging has focused on assessment and often quantitative measures of the apparent diffusion coefficient (ADC). Individual direction and trace weighted or combined direction DW images routinely manifest T2 effects, which complicate assignment of diffusion imaging behavior. This finding has been cited as limiting the utility and scientific validity of early techniques that have been used in evaluating the spine. In routine practice, it can be more useful to interrogate routine, combined, or trace diffusion images. These DW images additively combine T2 effects with diffusion alterations to significantly boost conspicuity (if not specificity) of lesions, which exhibit both diffusion restriction and T2 prolongation. As an example in the brain, although ADC values are lowest in the first few hours after stroke, it is only after T2 effects manifest that lesions are most conspicuous; when on (trace weighted) DWI the combined signal contributions manifest the characteristic light bulb high signal appearance. In contrast, chronic strokes have high diffusion values, which combine antagonistically with T2 prolongation to produce an isointense lesion. For clinical purposes, lower B values (eg, 500 s/mm 2 ) are typically used for spine imaging, allowing for significant T2 contribution to the trace-weighted DWI. Although in the interest of diffusion image purity, use of higher B values can effectively minimize T2 contribution; with clinically available techniques, the proportional tradeoffs in increased distortion and reduced SNR are effectively limiting. On the other hand, the synergistic contribution of combined T2 prolongation and diffusion restriction is likely responsible for some of the contributions made by DWI to the clinical MR imaging of spine disease discussed in this article.
Diffusion tensor imaging
Using a matrix of diffusion measurements in 6 or more unique directions, a mathematical model of diffusion in 3-dimensional space can be created providing an assessment of diffusivity in any arbitrary direction as well as the direction of maximum diffusivity. In the brain and spinal cord, individual white matter fiber tracts impose directionality (anisotropy) on water motion—diffusion is relatively free along fibers and restricted across fibers. Anisotropy is the extent to which the ordered white matter water motion (ellipsoid in shape) deviates from that of unrestricted, random water motion (spherical in shape). The direction of maximum diffusivity is a result of the tract orientation. The directionality of diffusion is conveyed by relative or fractional anisotropy and ranges from values of 0, representing isotropic diffusion, and 1 representing complete directional preference along the major diffusion eigenvector or direction. The rate of diffusion is represented by mean diffusivity (analogous to the ADC). Quantitative and qualitative assessment of anisotropy may yield important information as to white matter integrity and tract count that can give insight into a variety of disease states.
Clinical applications of DWI of the spine
One of the most rewarding extracranial applications of DWI is for the evaluation of the spine. DWI provides diagnostic value similar to that provided in the brain when assessing diseases of the spinal cord. DWI also can contribute to the detection and characterization of intradural-extramedullary, and epidural lesions as well. Perhaps the most fruitful extracranial contribution of DWI is for the evaluation of marrow disease.
Spinal cord lesions
Using conventional MR imaging techniques, the myriad appearance of intramedullary lesions can be insufficiently specific for definitive diagnosis. DWI may assist in the differentiation of etiology between inflammatory, neoplastic, and ischemia-related changes.
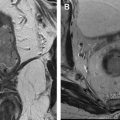
Neoplasm
Much as in the brain, DWI can be useful in the assessment of cord tumors. Primary cord tumors tend to be close to isointense with the normal spinal cord ( Fig. 7 ) as do metastatic lesions. When lesions are hemorrhagic ( Fig. 8 ) or exhibit a dense cellularity because of a high nuclear-to-cytoplasmic ratio, some hyperintensity on DWI will result ( Fig. 9 ). If dense cellularity or chronic blood products produce susceptibility effects on T2-weighted imaging, this can manifest as diminished signal on (particularly T2*-weighted EPI-based) DW images.