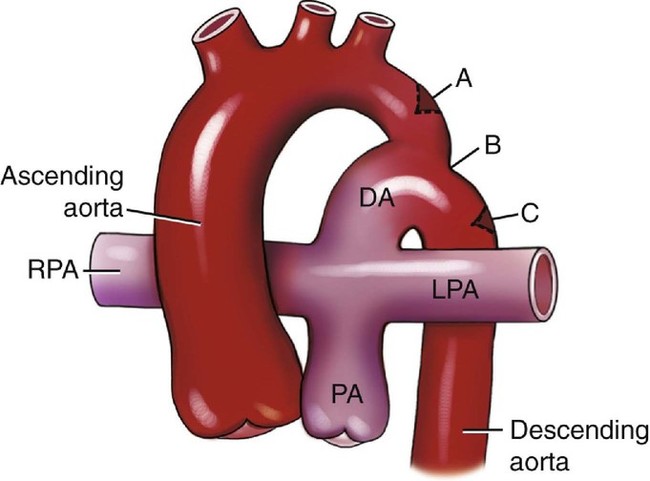
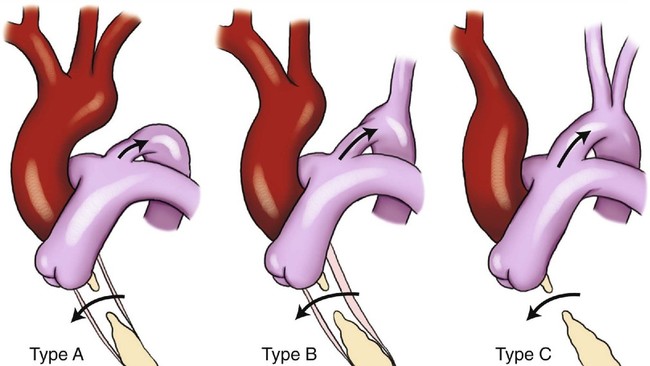
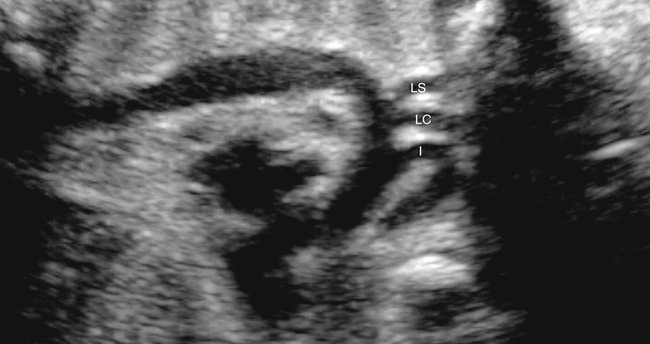
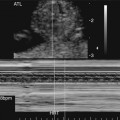
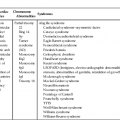
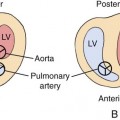
CHAPTER 11 Marisa R. Lydia and Julia A. Drose Coarctation of the aorta is a narrowing of a segment of the aortic lumen along the aortic arch, which results in an obstruction to blood flow. In more than 90% of cases, this narrowing is located between the origin of the left subclavian artery and the ductus arteriosus, also known as the aortic isthmus.1 The severity of the coarctation can range from a slight narrowing of the distal end of the arch to severe hypoplasia of the entire arch.2 Three types of coarctation are described according to the location of the aortic narrowing in relation to the ductus arteriosus (Fig. 11–1): • Preductal coarctation: narrowing occurring proximal to the ductus arteriosus • Ductal coarctation: narrowing occurring at the level of the ductus arteriosus • Postductal coarctation: narrowing occurring distal to the ductus arteriosus Ductal and postductal coarctations account for the remaining 98% of coarctations. They are usually an isolated finding, but an association with aortic valve abnormalities has been reported.3 Ductal and postductal coarctations occur as a result of the presence of abnormal muscular-ductal tissue. This type of coarctation occurs after birth when the ductus arteriosus closes. A surgical classification system of coarctation, based on the presence or absence of hypoplasia and the association of other intracardiac defects, was developed by Amato et al4 (Table 11–1). TABLE 11–1 Surgical Classification of Coarctation of the Aorta Adapted from Amato JJ, Galdieri RJ, Cotroneo JV: Role of extended aortoplasty related to the definition of coarctation of the aorta. Ann Thorac Surg 1991; 52:615–620. The most severe form of coarctation is termed “interruption of the aortic arch,” carrying a mortality rate of greater than 90% in the neonatal period if left untreated.5,6 Interruption of the aortic arch is usually classified into three types (Fig. 11–2)7: • Type A: interruption of the arch distal to the left subclavian artery • Type B: interruption of the arch between the left carotid artery and the left subclavian artery • Type C: interruption of the arch between the innominate artery and the left carotid artery The most commonly occurring form of aortic arch interruption is type B, with type C being the least common.7–10 Interruption of the aortic arch is also associated with numerous intracardiac defects. Coarctation is a primary developmental defect that results from abnormal development of the embryological left fourth and sixth aortic arches.11 Two theories have been proposed to explain the different types of coarctation. A preductal coarctation is thought to result from decreased blood flow through the left side of the fetal heart, resulting in impaired growth of the isthmus.12,13 This alteration in hemodynamics can occur as the result of an associated cardiac abnormality or from extracardiac impingement on the ascending aorta. In a fetus or neonate, the arch normally has a gradual tapering, with the smallest diameter of the arch occurring at the level of the isthmus.14 In utero, the diameter of the isthmus is approximately two thirds smaller than that of the ascending and descending portions of the aorta. After birth, the ductus arteriosus closes and the isthmus usually enlarges.15 The smaller size of the isthmus results from the fact that it is the segment of the arch through which the least amount of the combined cardiac output traverses.16 If blood flow is altered, resulting in the aorta receiving less blood than the ductus arteriosus and pulmonary artery, there may be even further reduction of flow through the isthmus, causing greater tapering of the arch. One example of this would be a decrease in left ventricular function because of premature narrowing of the foramen ovale. The resulting decrease in left ventricular size would lead to a decrease in left ventricular output and less blood traversing the region of the isthmus, thereby stunting its growth.17 A ductal or postductal coarctation is the result of the presence of aberrant ductal tissue in the aortic arch. This extra tissue causes a narrowing of the arch at the time of ductal closure, which results in decreased blood flow to the lower body.12 In utero, because of the presence of a patent ductus arteriosus, this aberrant tissue is usually inconsequential. Externally, a coarctation has a localized concavity on its posterolateral surface. Internally, the lumen is smaller because of asymmetry of the aortic wall. This eccentric shelf narrows the lumen from the superior wall opposite the orifice of the ductus arteriosus. As the ductus arteriosus closes, it increases the aortic obstruction by constricting the aortic orifice. There can be thickening of the wall within this area of narrowing. Proximal to the coarctation, the size of the arch may be normal or tubular hypoplasia may be present. Distal to the coarctation, the aortic wall is usually thin and dilated.7,15 Coarctation of the aorta accounts for 7% of all congenital heart defects.18 Coarctation as the primary cardiac lesion has a reported incidence of 6% prenatally. The incidence in stillbirths is 9%.18,19 These numbers may underestimate the true frequency because coarctations are common components of many types of complex congenital heart disease. Males are affected with coarctation two to three times as frequently as females.20–22 In 32% of cases, coarctation is an isolated anomaly. Sixty-eight percent of patients with coarctation have additional anomalies (Table 11–2). These anomalies involve the cardiovascular system (24%), genitourinary system (20%), central nervous system (12%), and skeletal system (6%).21,23,24 Familial coarctation has been reported in families and siblings. Siblings of an affected child have an occurrence risk estimated at 2%. This risk increases to 6% when two siblings are affected.24 A woman with a history of coarctation has a 4% chance of having an affected fetus. The risk is 2% when the father is the affected parent. Three percent to 5% of infants of diabetic mothers have coarctation. TABLE 11–2 Conditions Associated with Coarctation and Interrupted Aortic Arch When the diagnosis of coarctation is made in utero or in early infancy, it is easily correctable, but if it goes undetected, irreversible heart failure and acidosis can develop in the neonate.14,17 Unfortunately, the in utero diagnosis of coarctation can be extremely difficult because of the presence of the ductus arteriosus and the parallel circulation that exists before birth.13,25–27 Subtle changes associated with coarctation, such as a narrowing of the aortic arch, may not be apparent even when the arch is well visualized (Fig. 11–3).14,28 Indirect signs, such as discrepant ventricular size, with the right ventricle being larger than the left ventricle, are potentially useful for identifying fetuses at risk.13,14,29,30 However, as pregnancy progresses, the right heart becomes normally larger than the left. Therefore this finding is not as useful in the third trimester.30 Jung et al30
Coarctation of the Aorta
Definition
Type I
Coarctation with or without patent ductus arteriosus
IA
With ventricular septal defect
IB
With other major cardiac defects
Type II
Coarctation with isthmus hypoplasia, with or without patent ductus arteriosus
IIA
With ventricular septal defect
IIB
With other major cardiac defects
Type III
Coarctation with hypoplasia of isthmus and segment between left carotid and subclavian arteries, with or without patent ductus arteriosus
IIIA
With ventricular septal defect
IIIB
With other major cardiac defects
Embryology
Occurrence Rate
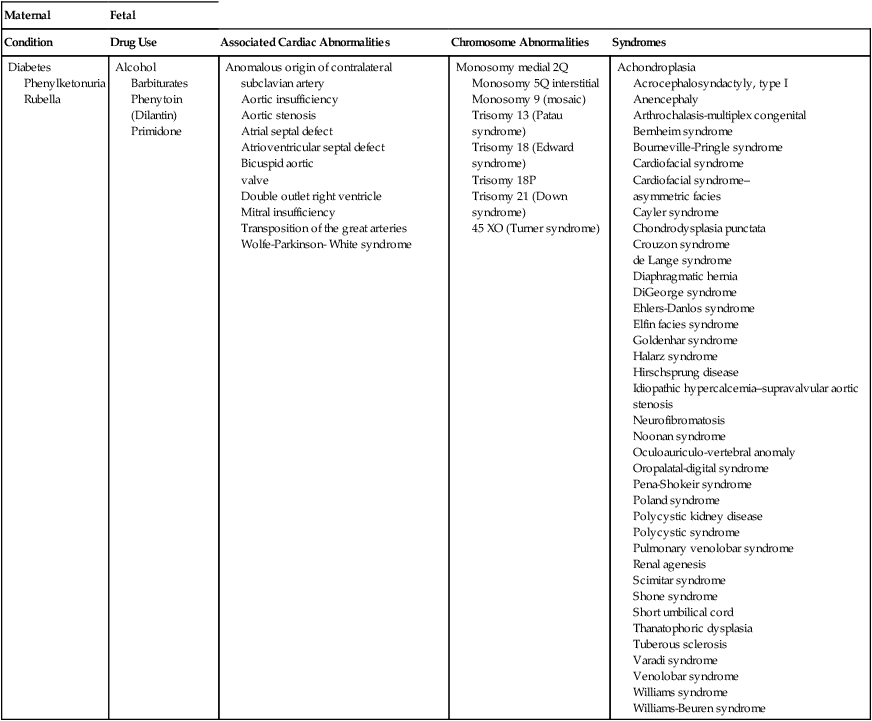
Maternal
Fetal
Condition
Drug Use
Associated Cardiac Abnormalities
Chromosome Abnormalities
Syndromes
Diabetes
Phenylketonuria
Rubella
Alcohol
Barbiturates
Phenytoin (Dilantin)
Primidone
Anomalous origin of contralateral subclavian artery
Aortic insufficiency
Aortic stenosis
Atrial septal defect
Atrioventricular septal defect
Bicuspid aortic
valve
Double outlet right ventricle
Mitral insufficiency
Transposition of the great arteries
Wolfe-Parkinson- White syndrome
Monosomy medial 2Q
Monosomy 5Q interstitial
Monosomy 9 (mosaic)
Trisomy 13 (Patau syndrome)
Trisomy 18 (Edward syndrome)
Trisomy 18P
Trisomy 21 (Down syndrome)
45 XO (Turner syndrome)
Achondroplasia
Acrocephalosyndactyly, type I
Anencephaly
Arthrochalasis-multiplex congenital
Bernheim syndrome
Bourneville-Pringle syndrome
Cardiofacial syndrome
Cardiofacial syndrome–
asymmetric facies
Cayler syndrome
Chondrodysplasia punctata
Crouzon syndrome
de Lange syndrome
Diaphragmatic hernia
DiGeorge syndrome
Ehlers-Danlos syndrome
Elfin facies syndrome
Goldenhar syndrome
Halarz syndrome
Hirschsprung disease
Idiopathic hypercalcemia–supravalvular aortic stenosis
Neurofibromatosis
Noonan syndrome
Oculoauriculo-vertebral anomaly
Oropalatal-digital syndrome
Pena-Shokeir syndrome
Poland syndrome
Polycystic kidney disease
Polycystic syndrome
Pulmonary venolobar syndrome
Renal agenesis
Scimitar syndrome
Shone syndrome
Short umbilical cord
Thanatophoric dysplasia
Tuberous sclerosis
Varadi syndrome
Venolobar syndrome
Williams syndrome
Williams-Beuren syndrome
Sonographic Criteria
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine