opacity to fine reticulation or coarse reticulation with honeycombing. Findings of pulmonary fibrosis (irregular reticulation, traction bronchiectasis, honeycombing) are seen on HRCT in about 10% of patients; ground-glass opacity is seen in 15%.
TABLE 14.1 Rheumatoid Arthritis | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
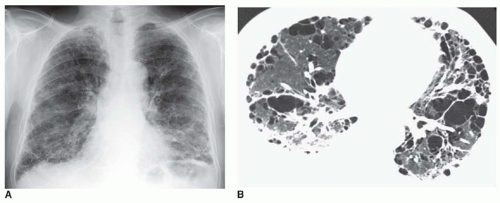 FIG. 14.1. Pulmonary fibrosis with honeycombing in a man with rheumatoid arthritis. A: Chest radiograph shows a coarse reticular pattern typical of honeycombing. Lung volume is reduced. B: Extensive honeycombing is visible on HRCT. This is a usual interstitial pneumonia pattern of lung disease. A right pleural effusion is also present. |
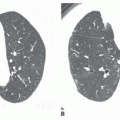
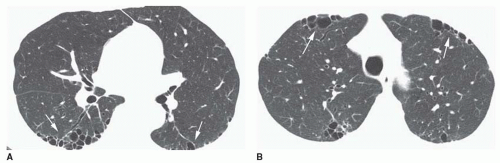 FIG. 14.2. Pulmonary fibrosis with honeycombing in a woman with rheumatoid arthritis. A: Patchy subpleural honeycombing (arrows) is visible in the posterior lung. B: Patchy honeycombing is also present in the upper lobes. Anterior upper lobe honeycombing (arrows) is more common in collagen-vascular diseases than in idiopathic pulmonary fibrosis. This may represent usual interstitial pneumonia or lymphoid interstitial pneumonia. |
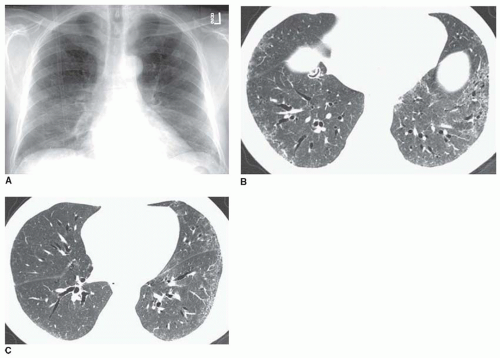 FIG. 14.3. Pulmonary fibrosis in rheumatoid arthritis with reticular opacities. A: Chest radiograph shows some reduction in lung volume and a mild nonspecific reticular abnormality at the lung bases. B: Fine reticular opacities are visible at the lung bases with evidence of traction bronchiectasis. There is no evidence of honeycombing. C: At a higher level, reticular opacities are less severe and predominate on the left. A distinct subpleural and lower lobe predominance is visible. This may be termed a nonspecific interstitial pneumonia or usual interstitial pneumonia pattern. |
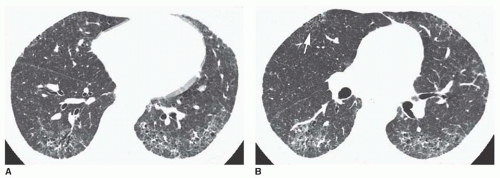 FIG. 14.4. Rheumatoid arthritis with reticular opacities and subpleural sparing. A: Fine reticular opacities are visible at the lung bases with evidence of traction bronchiectasis. Although there is a predominance in the subpleural lung, the immediate subpleural lung is less severely involved. This appearance tends to be associated with the histologic pattern of nonspecific interstitial pneumonia. B: At a higher level, subpleural sparing is also visible. Despite the absence of lower lobe honeycombing, patchy honeycombing is visible in the anterior upper lobe (arrow). This finding suggests a collagen-vascular disease. |
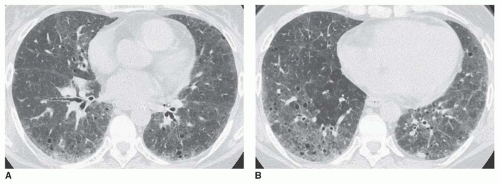 FIG. 14.5. Ground-glass opacity in a woman with rheumatoid arthritis. A: HRCT shows patchy ground-glass opacity with a subpleural predominance. B: The abnormality is more extensive at the lung bases. This appearance may reflect nonspecific interstitial pneumonia or lymphoid interstitial pneumonia (LIP). Small cystic lucencies are visible within the abnormal lung. These may represent traction bronchiectasis associated with lung fibrosis or cysts associated with LIP. |
are normal or show increased lung volumes. HRCT may show bronchiectasis, mosaic perfusion, and air trapping (see Fig. 14-7).
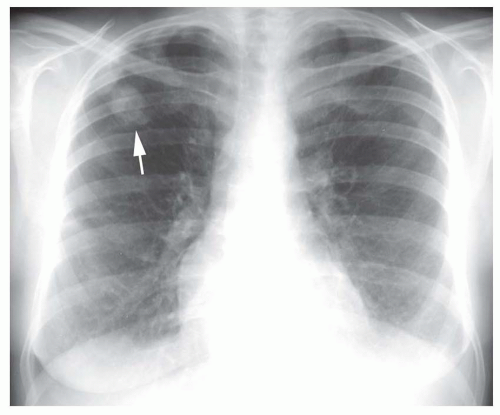 FIG. 14.6. Rheumatoid nodule. A young man with rheumatoid arthritis shows a well-defined nodule in the peripheral right upper lobe. Small pleural effusions are also present (arrow). |
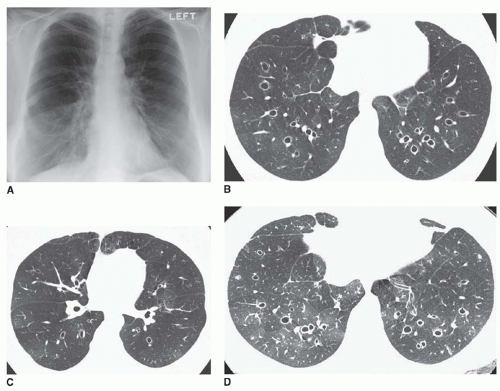 FIG. 14.7. Bronchiectasis and bronchiolitis obliterans in a young woman with rheumatoid arthritis. A: Chest radiograph shows large lung volume. B and C: HRCT scans at two levels show extensive bronchiectasis and regional differences in lung attenuation due to mosaic perfusion. D: Postexpiratory HRCT at the same level as (B) shows patchy air trapping typical of bronchiolitis obliterans. |
In early cases, ill-defined ground-glass opacity may be seen in the bases (Fig. 14-8A). With progression, reticulation may progress from fine to coarse, associated with progressive loss of lung volume.
TABLE 14.2 Scleroderma | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


