and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
8.1 Case 1: Incidentally Detected Villous Adenoma
History
A 55-year-old female patient who is being followed up with the diagnosis of lung carcinoma underwent 18F-FDG PET/CT scan for restaging.
Findings
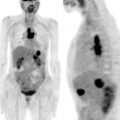
Fig. 8.1
MIP image (a) shows increased FDG uptake at left lung consistent with primary lung cancer. Axial slices of PET, CT, and fusion images (b–d) show hypermetabolic (SUVmax 7.4) soft tissue lesion at proximal rectum
Interpretation
Increased FDG uptake at proximal rectal lesion in soft tissue density is suspicious for villous adenoma.
Result
The lesion at rectum is resected and the histopathology revealed villous adenoma.
Teaching Point
Colonic adenomas constitute 70–80 % of all colorectal polyps, and they are considered a precursor of colorectal cancer. In a study 18F-FDG PET was found to have a true-positive rate of 83.3 % in detecting precancerous colonic adenomas.
8.2 Case 2: Metastatic Pulmonary Nodule and Villous Adenoma at Rectum in a Patient with Previous History of Lung Carcinoma
History
A 54-year-old female patient who had been treated for NSCLC underwent 18F-FDG PET/CT scan for restaging. Since a suspicious lung nodule was detected in the first procedure, 18F-FDG PET/CT scan is repeated 6 months later.
Findings
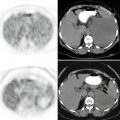
Fig. 8.2
Axial PET, CT, and fusion images (upper row) show a tiny pulmonary nodule at right lung located peripherally and showing subtle FDG uptake (arrow). There is a mass lesion at rectum (arrow) which creates a filling defect and exhibits significant FDG uptake (SUVmax 6.2) (second row)
Fig. 8.3
(a–c)18F-FDG PET/CT scan repeated 6 months after the first one (d–f) shows progression at pulmonary nodule in terms of both size and metabolic activity. Mass lesion at rectum also shows progression (arrows)
Interpretation
Hypermetabolic mass lesion in soft tissue density at rectum suspicious for villous adenoma. Pulmonary lung nodule is considered as a metastatic lesion.
Result
The lesion at rectum is resected and the histopathology revealed tubulovillous adenoma.
Teaching Point
Oral contrast agents provides better delineation of intestinal structures and mass lesions like villous adenomas. There is no significant difference between benign hyperplastic or precancerous lesions regarding SUVmax values, so when a hypermetabolic lesion causing filling defect is detected, colonoscopy should be performed.
8.3 Case 3: Initial Staging of Colorectal Carcinoma
History
A 72-year-old male patient with adenocarcinoma at sigmoid colon was referred to 18F-FDG PET/CT scanning for pretreatment staging.
Findings
Fig. 8.4
Axial CT and PET images display intensely increased FDG uptake at sigmoid colon (upper row) and focal hypermetabolic lesion at right lobe of liver (lower row)
Interpretation
Hypermetabolic lesion at sigmoid colon consistent with primary malignancy and metastatic focus at right lobe of liver.
Teaching Point
18F-FDG PET/CT is effective in the detection of liver metastases of colorectal carcinoma. On a per-patient basis the sensitivities of CT, MRI, and 18F-FDG PET/CT are found as 83.6 %, 88.2 %, and 94.1 % respectively.
8.4 Case 4: Initial Staging of Colorectal Carcinoma
History
A 74-year-old female patient who was diagnosed to have colorectal adenocarcinoma was referred to 18F-FDG PET/CT scanning for initial staging.
Findings
Fig. 8.5
Axial CT and fusion images show significantly hypermetabolic (SUVmax 14.3) mass lesion located at proximal ascending colon (upper row) and hypermetabolic lung nodule at lower zone of left lung (lower row)

Fig. 8.6
MIP image shows intensely hypermetabolic mass lesion at right lower quadrant of abdomen and multiple hypermetabolic foci representing lung nodules (arrows)
Interpretation
Primary malignant lesion at proximal ascending colon and multiple metastatic lung nodules.
Result
The patient underwent operation for malignant lesion at colon.
Teaching Point
18F-FDG PET/CT has limited role in diagnosis and initial staging of colorectal cancer. FDG PET is not effective in local and regional staging because of its limited spatial resolution. Current staging algorithms are mainly include surgical and pathologic data. Intense FDG uptake by the primary tumor, masks the pathological uptake at structures in vicinity resulting in a low sensitivity for detection of regional metastatic lymph nodes. 18F-FDG PET/CT may only be effective in pretreatment staging of patients who bear high risk for surgery.
8.5 Case 5: Initial Staging of Colorectal Carcinoma
History
A 28-year-old female patient with colorectal adenocarcinoma was referred to 18F-FDG PET/CT scanning for pretreatment staging.
Findings
Fig. 8.7
Axial CT and fusion images (a, b) display intensely increased FDG uptake (SUVmax 16) at rectum and pararectal lymph nodes with mild FDG uptake (SUVmax 4)
Fig. 8.8
Axial (a–c) and sagittal (d–f) PET, CT, and fusion images show intensely increased FDG uptake at rectum and pararectal lymph nodes showing mild FDG uptake and barely seen on PET images
Interpretation
Primary malignant lesion at rectum. Pararectal lymph nodes are metastatically involved but they are not clearly identified on PET images.
Result
The patient underwent operation for colorectal adenocarcinoma and lymph nodes turned out to be metastatically involved.
Teaching Point
Pararectal lymph nodes are not very well documented on PET images due to low FDG uptake because of micrometastatic invasion and obscuring effect of primary tumor which is in close proximity.
8.6 Case 6: Anal Cancer with Inguinal Lymph Node Metastasis
History
A 56-year-old male patient was diagnosed to have anal cancer and referred to 18F-FDG PET/CT scanning for pretreatment staging.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


