and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
16.1 Case 1: Ewing Sarcoma
History
A 26-year-old female underwent 18F-FDG PET/CT after having diagnosed as Ewing sarcoma with a biopsy from a mass lesion located at left sacroiliac region.
Findings
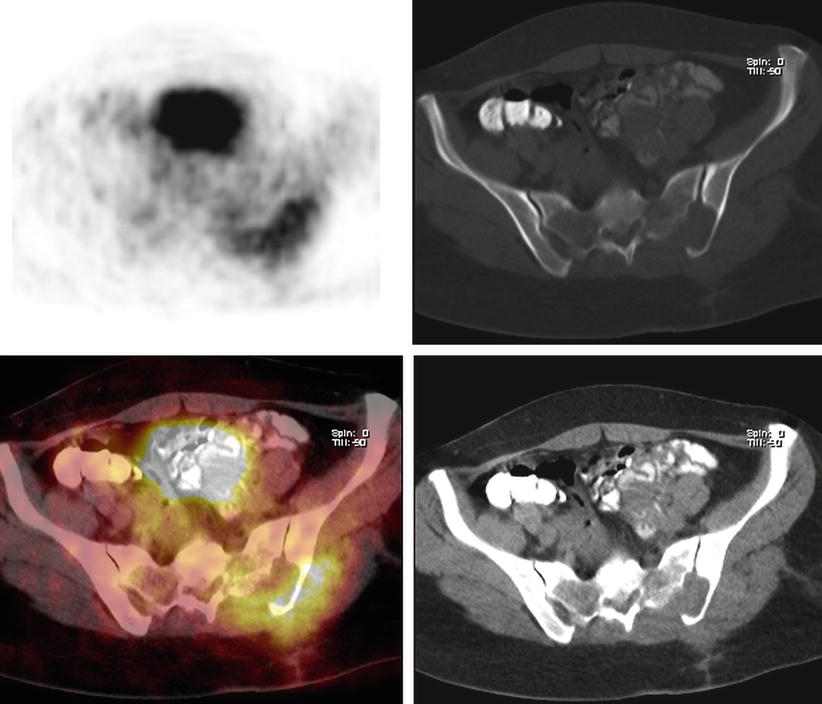
Fig. 16.1
Axial slices of CT, PET and fusion images show moderately hypermetabolic (SUVmax 5) mass lesion at left sacroiliac area invading gluteal muscles and obliterating sacral foramen

Fig. 16.2
MIP image
Interpretation
This finding is suggestive for malignant disease of bone invading surrounding structures.
Teaching Point
18F-FDG PET CT demonstrated high sensitivity and specificity in pretreatment staging of Ewing sarcoma and may provide additional information that modify therapy planning. It is proposed that FDG PET could replace bone scan when the initial evaluation of the extent of disease is concerned.
16.2 Case 2: Restaging of Ewing Sarcoma
History
A 17-year-old female who was diagnosed to have Ewing sarcoma 1 year ago is now being evaluated with 18F-FDG PET/CT for restaging, after having received chemotherapy and radiotherapy.
Findings
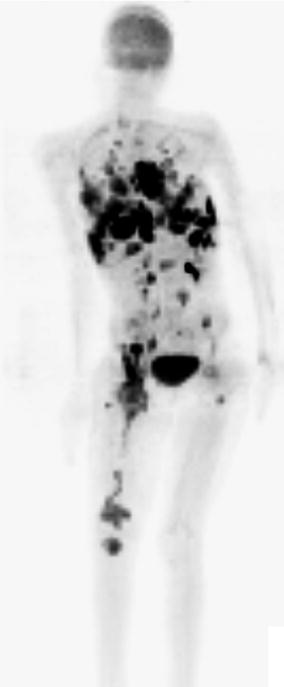
Fig. 16.3
MIP image shows multiple hypermetabolic lesions at pleural surfaces, lung parenchyma, mediastinal and intraabdominal lymph node stations, proximal and distal right femur, and proximal left femur (SUVmax 10)
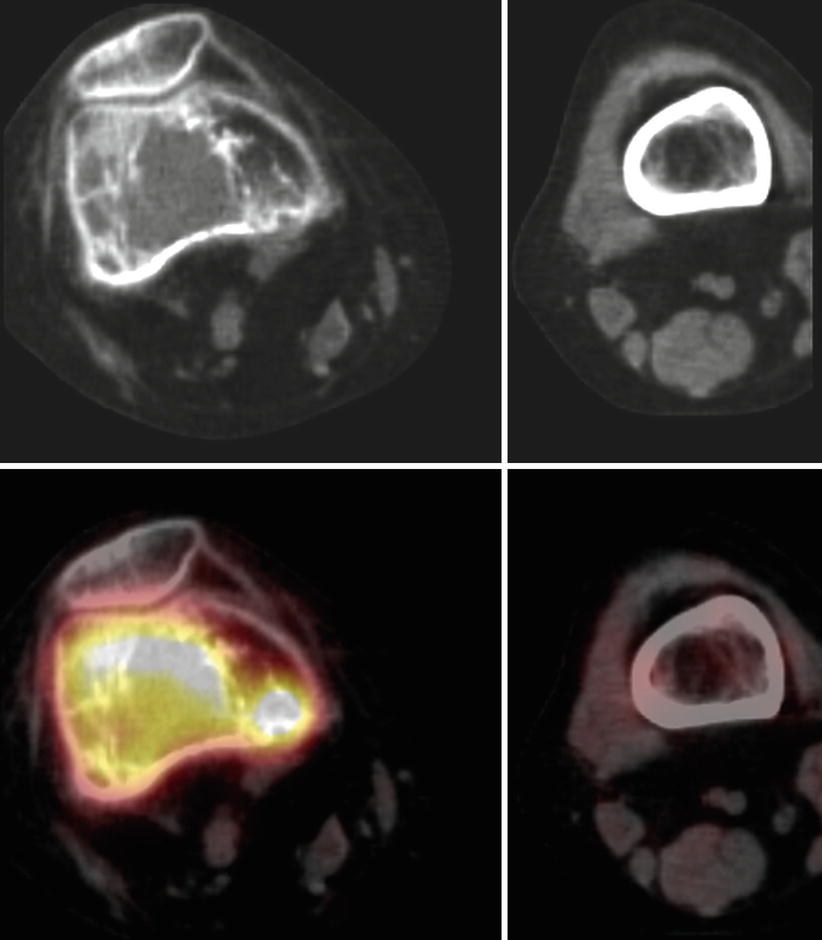
Fig. 16.4
Axial slices of CT and fusion images show increased FDG uptake corresponding to the lytic lesions at distal right femur
Interpretation
Multiple hypermetabolic lesions consistent with widespread metastatic disease.
Teaching Point
18F-FDG PET CT demonstrates high diagnostic accuracy for detecting recurrence in patients with primary skeletal Ewing sarcoma with a sensitivity of 95 % and a specificity of 87 %.
16.3 Case 3: Osteosarcoma
History
A 29-year-old female who was diagnosed to have osteosarcoma at left femur underwent 18F-FDG PET/CT.
Findings

Fig. 16.5
MIP image shows intensely hypermetabolic expansile mass lesion at distal left thigh (SUVmax 10.7) and linear FDG uptake proximal to this mass (SUVmax 6.4). There is also hypermetabolic mass lesion at hilar region of right lung (SUVmax 10)
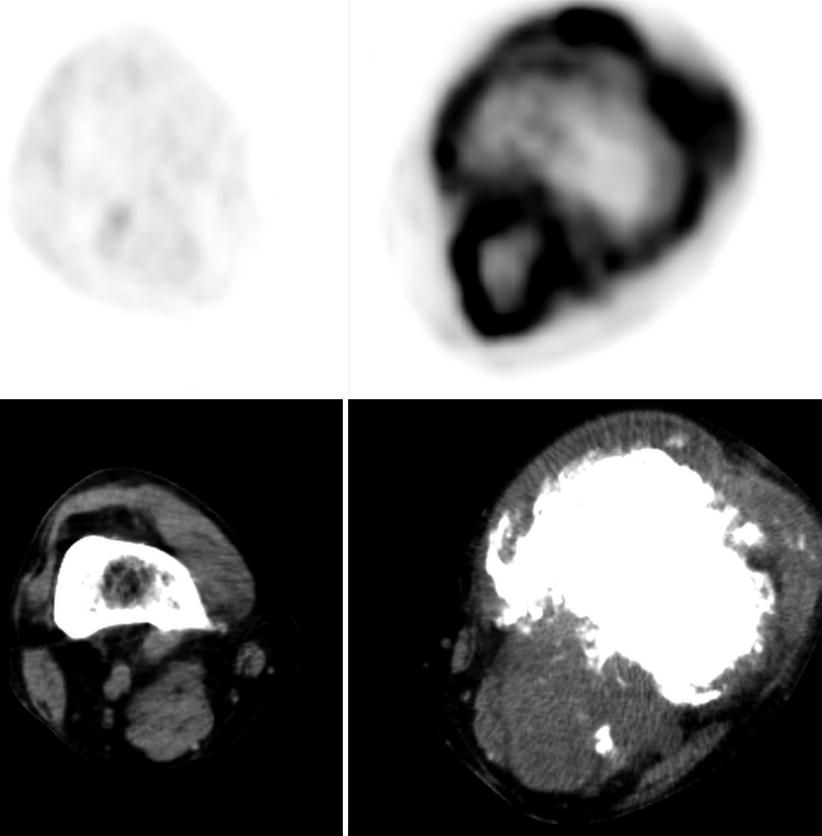
Fig. 16.6
Axial slices of PET and CT images show mass lesion at distal left thigh which shows bone destruction and involves calcified areas representing periosteal new bone formation. There is increased FDG uptake in circular fashion at mass lesion
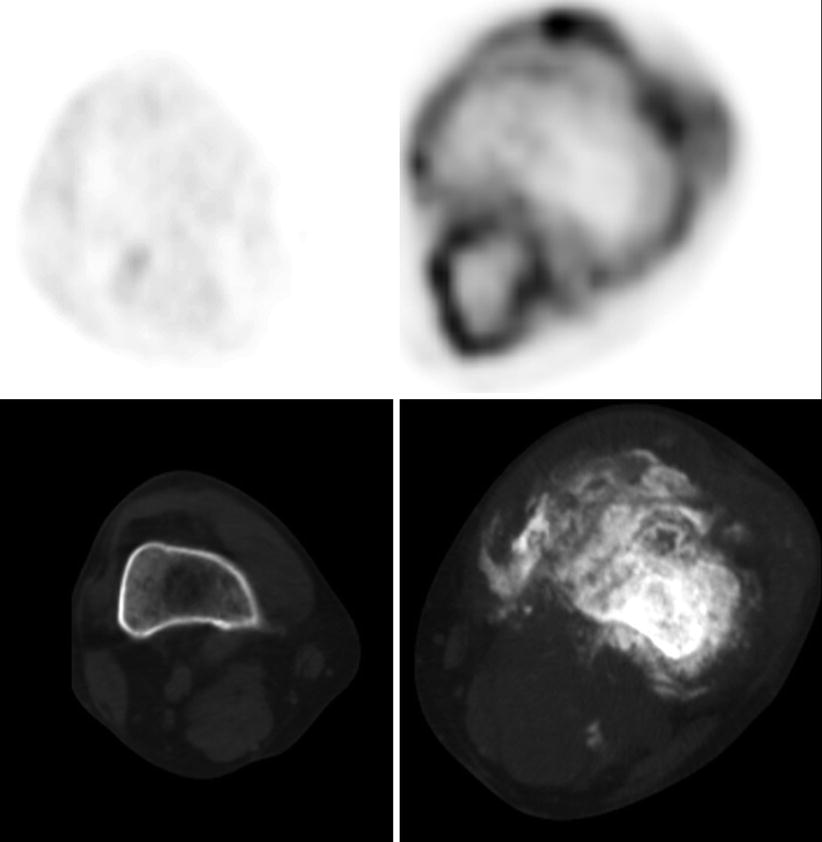
Fig. 16.7
Axial slices of PET and CT images show mass lesion at distal left thigh
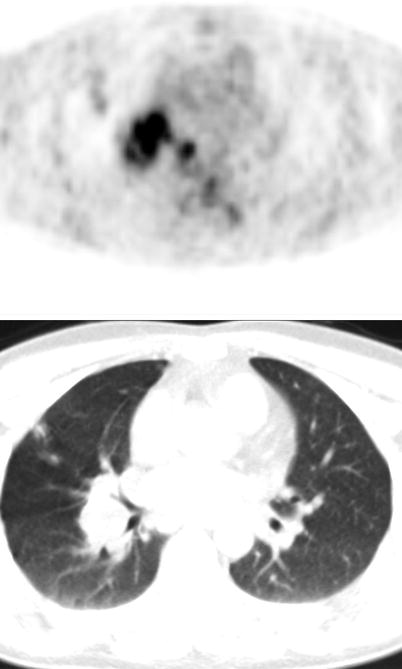
Fig. 16.8
Axial slices of PET and CT images show hypermetabolic mass lesion at right hilus
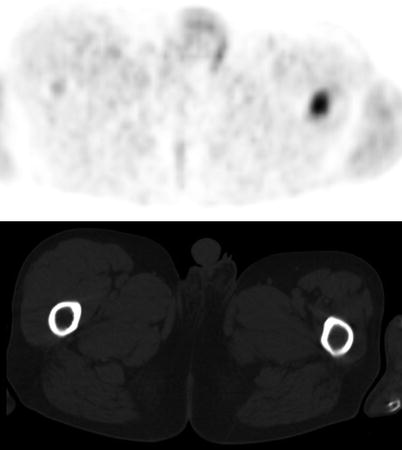
Fig. 16.9
Axial slices of PET and CT images display increased FDG uptake at diaphysis of left femur
Interpretation
Hypermetabolic mass lesion at distal left thigh is compatible with primary malignant disease of bone. A focal increased FDG uptake located at intramedullary femur diaphysis above the primary lesion representing skip metastasis is seen. Right hilar lesion with FDG uptake is consistent with pulmonary metastasis.
Teaching Point
Although, for osteosarcoma, FDG PET is less sensitive than bone scan for the detection of bone metastases and accuracy in detecting pulmonary metastases is lower than CT, bone and lung lesions in this case are correctly identified by PET.
16.4 Case 4: Solitary Plasmocytoma
History
A 67-year-old male status post cervical vertebral body biopsy proven to be solitary plasmacytoma underwent 18F-FDG PET/CT.
Findings
Fig. 16.10
Lateral MIP image (a), axial slices of PET, fusion, and CT images (b–d) shows moderately hypermetabolic lesion destructing vertebral body and invading posterior elements of vertebra. There is not any other pathological FDG uptake at whole body PET images
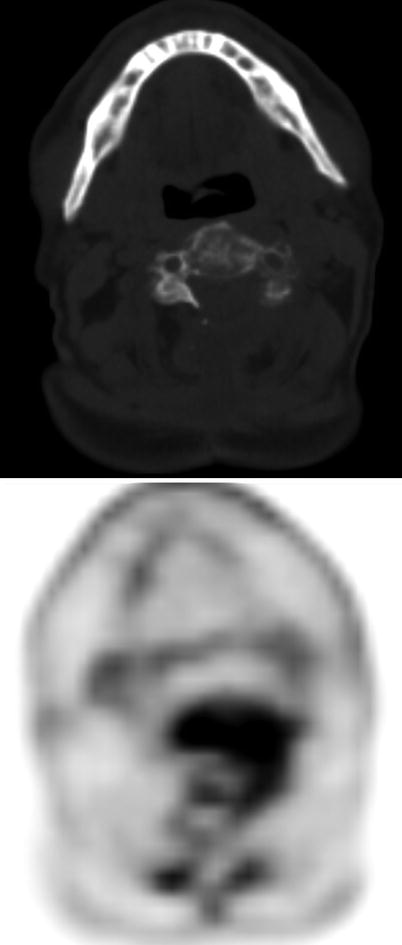
Fig. 16.11
Axial slices of CT and PET display hypermetabolic lesion destructing vertebral body
Interpretation
Solitary plasmocytoma involving vertebral body. Moderate FDG uptake at lesion is an expected finding for plasmocytoma.
Teaching Point
18F-FDG PET/ CT has a high performance for initial staging of plasmacytoma (98 % sensitivity, 99 % specificity). It has the advantages of performing whole-body examinations with the ability of detecting medullary and extramedullary lesions in one single examination.
16.5 Case 5: Plasmocytoma
History
A 57-year-old male who had the diagnosis of plasmocytoma underwent 18F-FDG PET/CT for pretreatment staging.
Findings
Fig. 16.12
Axial CT and PET images (a, b) show intensely hypermetabolic soft tissue lesion at right retroorbital area. MIP image (c) shows multiple moderately active randomly distributed pathologic hypermetabolic foci within the bony structures
Interpretation
This is consistent with extensive active multiple myeloma.
Teaching Point
Solitary plasmocytoma may be a local manifestation of multiple myeloma and 18F-FDG PET CT may detect other unsuspected sites of bone involvement which are overlooked at other conventional imaging methods.
16.6 Case 6: Multiple Myeloma
History:
A 63-year-old male who was diagnosed to have multiple myeloma underwent 18F-FDG PET/CT for pretreatment staging.
Findings
Fig. 16.13
Axial PET and CT images (a, b) show intensely hypermetabolic foci corresponding to lytic lesions at pelvic bones. MIP image (c) shows numerous foci of increased FDG uptake at bony structures
Fig. 16.14
Axial CT and PET images show increased FDG uptake at lytic lesions at vertebral body (a, b) and rib (c, d) (arrows)
Interpretation
This is consistent with extensive active multiple myeloma.
Teaching Point
18F-FDG PET CT finds additional unanticipated bone lesions and upstage the patients in 33–43 % of multiple myeloma cases.
16.7 Case 7: Sacrococcygeal Chordoma
History
A 57-year-old female underwent 18F-FDG PET/CT for characterization of sacrococcygeal mass detected on CT.
Findings
Fig. 16.15
Sagittal PET, CT, fusion (a–c) and axial fusion, PET, and CT (d–f) images show destructive mass at sacrococcygeal region and faint FDG uptake within the mass is observed
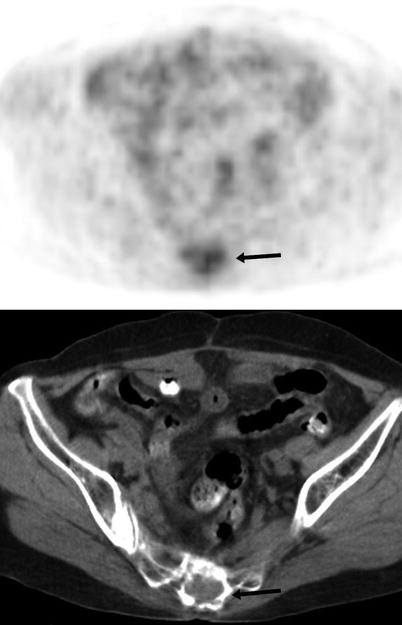
Fig. 16.16
Axial PET and CT images show subtle FDG uptake at sacrococcygeal region accompanying the destructive mass (arrow)
Interpretation
Although the metabolic activity of the mass is subtle, the lesion is suspicious for malignancy when location and destructive nature is concerned.
Result
The patient underwent surgery and histopathology revealed sacrococcygeal chordoma.
Teaching Point
Chordoma is a rare malignant bone tumor derived from notochordal rests, and the most common site is the sacrococcygeal region. Chordomas are not FDG avid tumors, so chordoma should be considered when an osteolytic mass in the sacral region on FDG PET/CT is encountered, even if its metabolism is low.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


