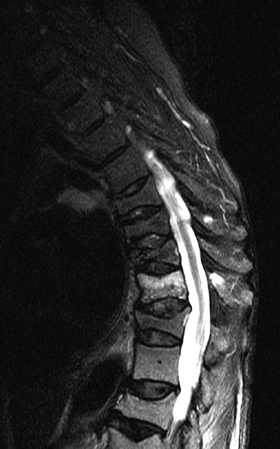
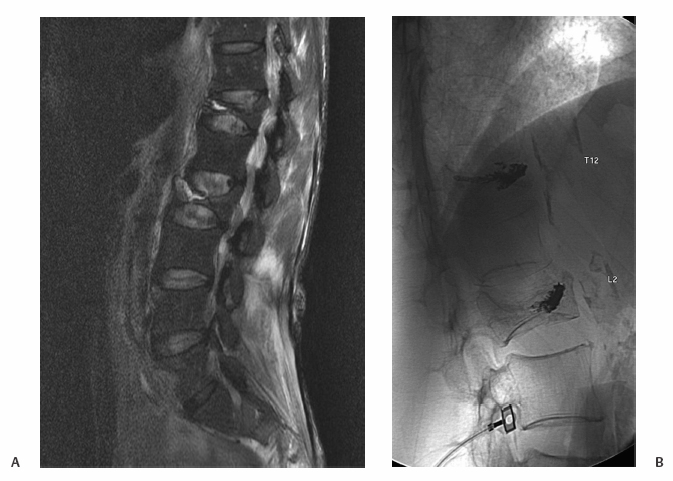
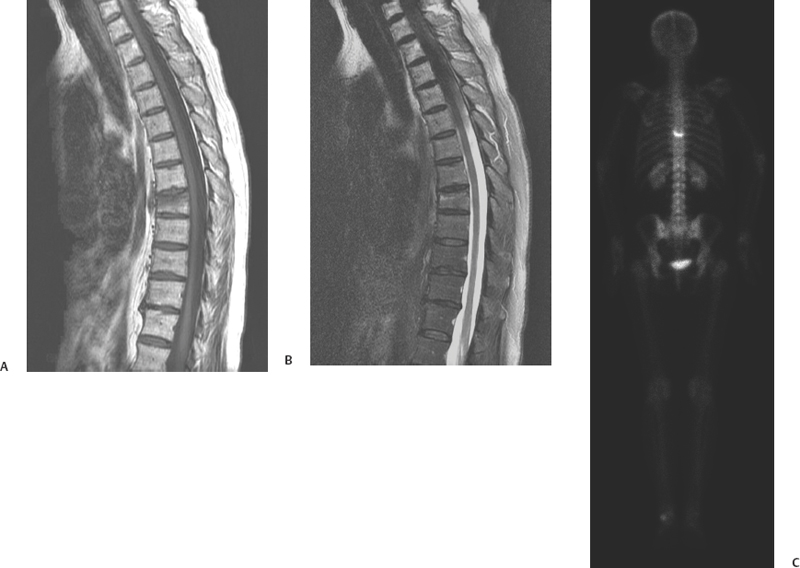
20 Compression Fractures: Vertebroplasty David F. Kallmes The care of patients suffering from painful, osteoporotic vertebral fractures has been revolutionized by the development of percutaneous vertebroplasty. Prior to the era of vertebroplasty, these patients usually were managed using a combination of analgesics, bedrest, and bracing. The attendant morbidity of these measures was essentially unavoidable because surgical intervention was rarely, if ever, undertaken. Watchful waiting and suffering was the typical scenario for patients with painful, osteoporotic vertebral fractures. Percutaneous vertebroplasty comprises the injection of medical polymers or cements, usually polymethylmethacrylate (PMMA), into a fractured vertebra. Initially used in spinal tumors in France in the 1980s,1 the technique was applied to osteoporotic fractures by Dion and Jensen at the University of Virginia in 1993. In a small series of patients published in 1997, these latter authors noted improvement in pain in 90% of patients, with little procedure-related morbidity.2 The procedure has disseminated rapidly throughout the United States in the past decade for several reasons. First, at the time this procedure became commonly offered, there were no satisfactory alternative therapies. Second, the procedure is fairly easy to perform. Third, the apparent efficacy as reported in numerous reports is outstanding. Last, Medicare currently reimburses for the procedure in most areas of the country. Upwards of 80,000 vertebroplasty procedures are performed annually, and most likely the numbers of procedures will only increase in the future. Vertebroplasty is typically offered to patients suffering from painful, spontaneous, vertebral compression fractures, usually resulting from systemic osteoporosis. In the majority of such patients, pain will relent within 6 to 8 weeks, so many vertebroplasty practitioners will recommend delaying the procedure until pain persists for at least 6 weeks. It remains unclear why a subset of patients fails to achieve spontaneous regression of pain from osteoporotic fractures, but this subset is the most appropriate group of patients to offer vertebroplasty and the one most likely to benefit from this procedure. Patients with compression fractures due to osteoporosis typically complain of midline back pain that is severe and worsens with activity. In the mid- and upper thoracic region, patients also complain of radicular-type pain with radiation around the rib cage. In the lumbar region, especially with severe fractures, there may be some component of radicular pain. However, signs or symptoms that suggest spinal cord compression are considered contraindications to vertebroplasty.3 Most patients are maintained with oral analgesics, often narcotics, for control of the associated pain. Thus, it may be useful to instruct referring physicians to have the patients hold their analgesics on the day that they present for a vertebroplasty evaluation so that pain patterns are not masked by their pain medication. In this group of patients, physical examination often elicits pain on palpation over the spinous process of the affected vertebra or vertebrae.2 However, such a physical finding is not required for offering the procedure; patients without pain on palpation over the fracture may still gain relief from vertebroplasty.4 In patients with a clear-cut history and with a plain radiograph showing a new vertebral compression fracture, it is reasonable to proceed directly to vertebroplasty without other imaging modalities. In practice, however, the majority of patients being considered for vertebroplasty will have other spinal imaging performed. Commonly, a magnetic resonance imaging (MRI) scan will be performed as it has been found to be useful in several scenarios. Patients with multiple fractures of varying age can pose a problem for an interventionalist who may find it difficult to identify the fracture or fractures responsible for the patient’s pain. Most practitioners consider the finding of marrow edema on MRI as a marker for a painful vertebra, so all edematous fractures will likely be treated and nonedematous fractures would not be treated (Fig. 20.1). However, there remains no good study to prove the hypothesis that marrow edema indicates a pain-generating fracture; and vertebrae with normal marrow signal, without edema, have also shown good response to vertebroplasty.5 Intraosseous cavities or clefts, historically considered as Kümmell osteonecrosis, are readily identified on MRI and can be a target for cement infusion (Fig. 20.2).6 Another potential strength of MRI is that it can allay fears of an underlying neoplasm and can assess for compression of the spinal canal or nerve roots. MRI can also assess for related pain-generating lesions such as spinal stenosis and disk pathology. Patients who cannot undergo MRI are often referred for bone scanning. At least one series of patients treated based on elevated activity on bone scan showed good relief following vertebroplasty.7 A bone scan may be more physiologically relevant than an MRI because uptake on bone scan indicates ongoing bone turnover in a healing fracture, whereas MRI simply shows edema (Fig. 20.3). However, the anatomic detail offered by a bone scan is substantially inferior to MRI, and often exact identification of abnormal levels may be difficult on bone scan imaging, especially in the upper thoracic region. Other imaging modalities such as computed tomography are rarely performed as part of a workup prior to vertebroplasty, but may be useful to assess the integrity of the posterior cortex of the involved vertebral body. Fig. 20.1 A 79-year-old woman with severe midthoracic back pain and multiple thoracic compression fractures. Sagittal T2-weighted magnetic resonance image shows high-signal edema within the compression fracture at T10, while multiple other fractures show no edema. Patient underwent T10 vertebroplasty with good result. Fig. 20.2 A 56-year-old man with severe back pain. (a) Sagittal T2-weighted magnetic resonance image shows severe compression fractures at T12 and L2. At both levels there are fluid-filled cavities within the verebral bodies, indicating osteonecrosis. (B) Postvertebroplasty radiograph shows barium-opacified polymethylmethacrylate (PMMA) at both levels. Fig. 20.3 A 70-year-old woman with severe back pain. (A) Sagittal T1-weighted and (B) T2-weighted magnetic resonance images show mild edema under the superior endplate at T9. (C) Anteroposterior image from radionuclide bone scan shows intense uptake at T9. Patient improved following T9 vertebroplasty. All patients presenting with spontaneous vertebral fractures and osteopenia should be evaluated for osteoporosis. Indeed, medical treatment of osteoporosis should be initiated because it can reduce the risk of a new fracture by 50% or more. Therefore, all patients should be counseled that, while vertebroplasty can potentially alleviate current pain, optimal care must include treatment of their underlying osteoporosis. Any patient with a suspected systemic infection should be fully evaluated prior to vertebroplasty because instillation of PMMA in the setting of bacteremia could lead to seeding of the cement. Infection of PMMA in vertebroplasty, though rare, may lead to the need for vertebrectomy.8 It is also prudent to assess for a potential coagulopathy and to hold anticoagulants and antiplatelets, except aspirin, during the periprocedural period.9 Vertebroplasty is usually performed under fluoroscopic guidance and many busy centers perform the procedure in a dedicated, biplane angiography suite with high-quality fluoroscopic imaging. Patients are placed in the prone position and are administered intravenous sedation and analgesics. Rarely, for underlying comorbidities such as pulmonary compromise, is vertebroplasty done under general anesthesia.
Patient Selection
History and Physical Examination
Imaging
Laboratory Evaluation
Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


