Congenital Thoracic Diseases and Malformations
The lungs, airways, and pulmonary vessels are involved in several developmental anomalies. There is no uniform system for classification of such developmental anomalies. A breakdown into malformations affecting the airways, vascular architecture, or a combination of both has been proposed.1 The disease entities presented in ▶Table 19.1 are classified according to that system.
19.1 Congenital Lobar Emphysema
Congenital overinflation of a lung lobe is known as congenital lobar emphysema or, more pathogenetically accurate, as congenital lobar overinflation. Frequent causes include abnormal softening of the bronchial cartilage, its complete absence, or external compression of the lobe bronchus (e.g., because of a bronchogenic cyst or pulmonary artery).2 In almost half of all cases, the disease involves the left upper lobe, followed by the middle lobe.
Type I: in infants, the most severe form, causes early respiratory distress.
Type II: in older children, with milder symptoms.
Type III: in adults or older children, asymptomatic incidental finding.
Types II and III are rare.
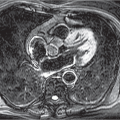
On imaging, the diseased lobe appears enlarged and hyperlucent (▶Fig. 19.1). If diagnosis is not made during the first month after birth, it may be difficult to distinguish congenital lobar emphysema from Swyer-James syndrome but the latter is not always strictly confined to a single lobe.
19.2 Bronchial Atresia
Bronchial atresia is a rare malformation where the bronchus of a lobe, segment, or subsegment is not fully formed. That implies discrete occlusion of the bronchial lumen.5 Distal to the atresia, the bronchus may be filled with mucus and dilated. Overinflation of the affected lung regions is markedly less pronounced than in congenital lobar emphysema and is caused by air admitted via collateral ventilation from adjacent lung areas. Bronchial atresia is often asymptomatic and identified only as an incidental finding on imaging. Surgical resection of the diseased lung regions is indicated if it causes recurrent pulmonary infections.
| ||||||||||||
19.3 Congenital Pulmonary Airway Malformation
Congenital pulmonary airway malformation (CPAM) was previously known as congenital cystic adenomatoid malformation of the lung. The current term is more accurate since only three of the five histologic types of CPAM are of a cystic nature and only one contains adenomatoid components.6 Depending on the histologic type, it involves developmental anomalies at different levels of the tracheobronchial system ranging from the trachea to major bronchi to the alveolar ducts or distal acini.2
Imaging is unable to differentiate the histologic types. Instead, these are classified into three categories based on the cyst size (Table 19.2). The cystic structure of types I and II is routinely identified on CT, but the type III microcystic structure is not. The latter is included in the differential diagnosis of solitary pulmonary nodules and has no pathognomonic radiologic features. The types I and II cysts associated with CPAM can be connected with the bronchial system, in which case they may be purely air filled or contain air-fluid levels (▶Fig. 19.3). They become completely filled with fluid in the absence of bronchial drainage (▶Fig. 19.4). The small-cystic type II, in particular, may occasionally have
abnormal systemic blood supply. In that respect, it is similar to sequestration. These hybrid lesions exhibit radiologic features of both entities (▶Fig. 19.5).5
abnormal systemic blood supply. In that respect, it is similar to sequestration. These hybrid lesions exhibit radiologic features of both entities (▶Fig. 19.5).5
Often, CPAM constitutes an incidental imaging finding. At times, it becomes symptomatic because of recurrent pulmonary infections or because of its size and space-occupying effect.2 Elective resection should be considered due to the potential susceptibility to malignant transformation.7
 Fig. 19.1 Congenital lobar emphysema in the left upper lobe of infant. CT image. Hypodensity and overinflation of the left upper lobe causing mediastinal shift to the right. Normal density of the left lower lobe apex (arrow). |

19.4 Bronchogenic Cysts
Bronchogenic cysts are caused by an embryonic developmental anomaly of the tracheobronchial tree branching.2 These are found most commonly in the mediastinal region close to the tracheal bifurcation and are less frequently seen in the lung parenchyma, in the vicinity of the pleura or diaphragm.8
Occasionally, the cysts cause recurrent infections; then their resection is indicated.2 Otherwise, asymptomatic bronchogenic cysts are incidental findings.
Occasionally, the cysts cause recurrent infections; then their resection is indicated.2 Otherwise, asymptomatic bronchogenic cysts are incidental findings.
Table 19.2 Radiologic types of congenital pulmonary airway malformation1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


