- •
Free-breathing 3D coronary MR angiography allows for visualization of all major coronary arteries without administration of contrast medium or radiation exposure to the patient.
- •
Acquisition of free-breathing whole heart coronary MR angiography requires imaging time of 5 to 20 minutes.
- •
Whole heart coronary MR angiography permits noninvasive detection of significant coronary artery disease, with a sensitivity of greater than 80% and specificity of greater than 90% in single center studies.
- •
Coronary MR angiography provides noninvasive detection and size measurement of coronary artery aneurysms in patients with Kawasaki disease.
- •
Coronary MR angiography is well suited for assessing coronary artery disease in patients with renal failure, because no contrast administration is required.
- •
Coronary MR angiography is useful in evaluating stenosis of the coronary arterial lumen in patients with heavy coronary calcification.
- •
32-channel cardiac coils can provide substantial reduction of imaging time of whole heart coronary MR angiography with higher study success rate.
- •
High-resolution 3D coronary MRA images can be obtained with 3-Tesla MR imagers if images are acquired after contrast.
- •
Phase contrast cine MR imaging is useful for the functional assessment of the stenoses in coronary artery bypass grafts.
CORONARY MR ANGIOGRAPHY
Catheter X-ray coronary angiography has been used as the gold standard for identifying significant luminal narrowing of the coronary arteries. However, a considerable number of patients undergoing elective catheter coronary angiography are found to have no significant coronary arterial disease. Consequently there is a strong need for a noninvasive test that can reliably delineate narrowing of the coronary arteries. Contrast enhanced multislice CT is now widely used as a noninvasive method that can provide reliable exclusion of the coronary artery disease. From a patient’s point of view, however, coronary MR angiography is more preferable to coronary CT angiography in screening coronary artery disease, because it does not expose the patient to radiation or necessitates a rapid injection of iodinated contrast material.
Noninvasive imaging of the coronary artery with MR angiography is technically challenging, because of small size of the vessel, complex motion caused by cardiac contraction and respiration, and substantially slower data acquisition speed by CMR as compared with multislice CT. In recent years image quality, volume coverage, and acquisition speed of 3D coronary MR angiography were substantially improved, permitting the acquisition of high-quality 3D MR angiograms encompassing the entire coronary arteries within a reasonably short imaging time.
Free-breathing 3D coronary MR angiography acquired with respiratory and electrocardiographic gating is currently the most commonly used MR approach for the assessment of coronary arteries in patients with heart disease. Respiratory gating is achieved by using a navigator echo method that measures the position of the right lung-diaphragm interface by using the MR signal. Electrocardiographic gating is also used to acquire image data during the rest period of the coronary artery in the cardiac cycle. Steady-state free precession sequences permit acquisition of 3D coronary angiograms that encompasses the entire heart with high blood contrast. By using a “whole heart coronary MR angiography” approach, one can visualize all three major coronary arteries without administration of contrast medium or radiation exposure to the patient ( Figures 23-1 and 23-2 ). Imaging time of whole heart coronary MR angiography ranged between 5 to 20 minutes.


Detection of Coronary Artery Disease with MR Angiography
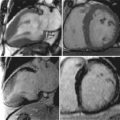
Whole heart coronary MR angiography has been shown to be useful for the detection of significant coronary artery disease, with the sensitivity and specificity similar to those by 16-slice multislice CT in recent studies ( Table 23-1 , Figures 23-3 and 23-4 ). Coronary MR angiography may be useful for the diagnosis of:
- •
Coronary artery anomalies
- •
Coronary artery aneurysm in patients with Kawasaki disease
- •
Coronary arterial stenoses in patients with renal failure.
- •
Coronary arterial stenoses in patients with heavy calcification.
- •
Screening coronary artery disease in asymptomatic subjects and those with low likelihood of coronary artery disease.
| MODALITY | SENSITIVITY | SPECIFICITY | STUDY |
|---|---|---|---|
| Whole-heart coronary MR angiography | 78% | 96% | Sakuma H: J Am Coll Cardiol 2006;48:1946. |
| 78% | 91% | Jahnke C: Eur Heart J 2005;26:2313. | |
| Multislice CT | 76% | 95% | 16-slice CT ( n = 826, metaanalysis) |
| Hamon M: J Am Coll Cardiol 2006;48:1896. | |||
| 87% | 96% | 40–64-slice CT ( n = 536, metaanalysis) | |
| Hamon M: J Am Coll Cardiol 2006;48:1896. |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


