Fig. 28.1
Development of cardiac veins. Posterior drawings of the embryonic heart at 4 weeks (a) and well-developed heart (b) at 8 weeks. The right and left anterior cardinal veins connect through small anastomotic veins which form the left brachiocephalic vein. The right horn of the sinus venosus and the cardinal veins eventually form the posterior wall of the right atrium (RA) and the vena cava, respectively. The left sinus horn regresses and loses its connection with the left anterior cardinal vein and becomes the coronary sinus (CS) and the oblique vein of left atrium (Marshall). Angiogenic sprouts (small asterisks in a) of the sinus venosus covering the epicardial surfaces (shown by red curved arrows) turn into the coronary vessels including veins (colored in dark green). GCV great cardiac vein, IVC inferior vena cava, SVC superior vena cava, LAA left atrial appendage
It was suggested in earlier experiments that coronary vessels arise from the proepicardium, a transitory structure in the embryonic heart that forms epicardium and several internal tissues [3]. Recent histological analysis in mouse and cardiac organ culture has shown that coronary vessels arise from angiogenic sprouts of the sinus venosus, the major vein that returns circulating blood to the embryonic heart [4]. Some sprouting venous endothelial cells dedifferentiate into arteries and capillaries as they invade the myocardium and some remain on the surface and differentiate into veins [4].
Cardiac Vein Classification
A complete, highly efficient and clinically useful classification of the CVS is not as straightforward as in the case of the coronary arteries. The epicardial coronary veins depict a very different macroscopic disposition, as compared to the coronary arterial system, and show many more individual variations.
Modern anatomical classification divides the cardiac veins into two main groups including tributaries of the Greater-Cardiac Vascular System (CVS) and tributaries of the Smaller-CVS, consisting of the Thebesian vessels [5–7]. For clarity Greater-CVS is divided into two groups including CS and non-CS tributaries (Fig. 28.2). Branches of the two systems can communicate. The term Compound-CVS has been used to describe structures in which venous drainage is performed equally by both systems (Fig. 28.2) [6].
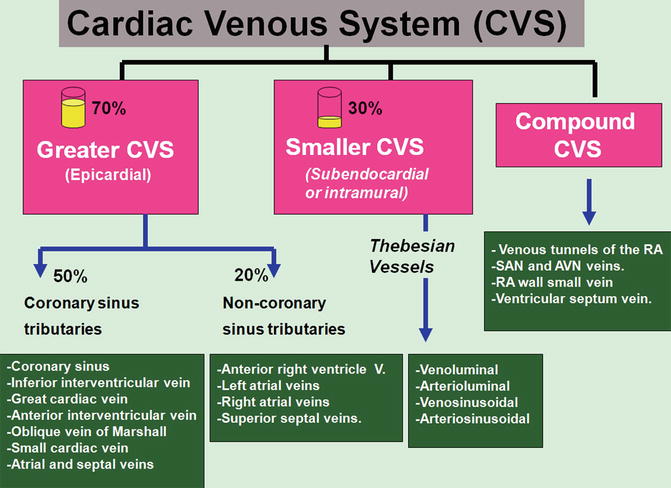
Fig. 28.2
Classification of the cardiac venous system (CVS), right atrium (RA), sinuatrial node (SAN), atrioventricular node (AVN), vein (V)
In ventricular myocardium, the external two thirds are drained by the Greater-CVS, and the internal third is mainly drained by tributaries of the Smaller-CVS [6].
The left ventricle and part of the right ventricle and the left atrium (LA) are drained by the CS tributaries, and the majority of the right ventricle and both atria are drained by the non-CS tributaries. Almost all veins of the Greater-CVS are finally drained into the right atrium. In the right atrium, the wall of sinus venosus is drained by tributaries of the Greater-CVS, and the right atrial appendage is mainly drained by the Smaller-CVS [8].
Smaller-CVS (Thebesian Vessels)
Consisting of sinusoids, channels, and lacunae, this subendocardial and intramyocardial bidirectional communicating network runs in every direction conducting blood from epicardial coronary arteries into the cardiac chambers and provides myocardial nourishment (Fig. 28.3). Sinusoids are large capillaries with different morphologies (Figs. 28.4 and 28.5). They are remnant of the primitive cardiac circulation.
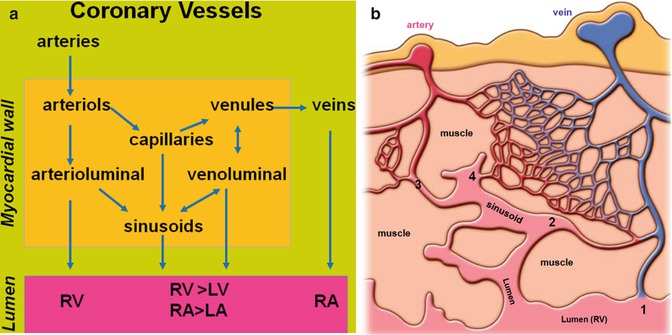
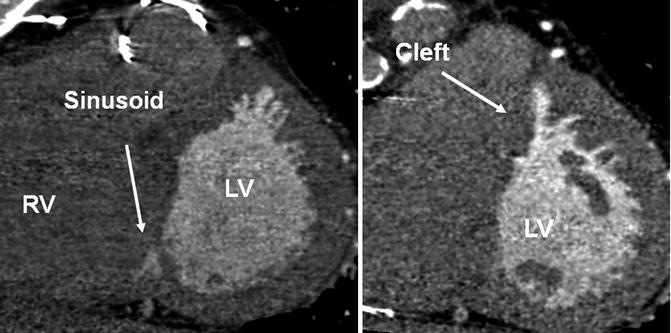
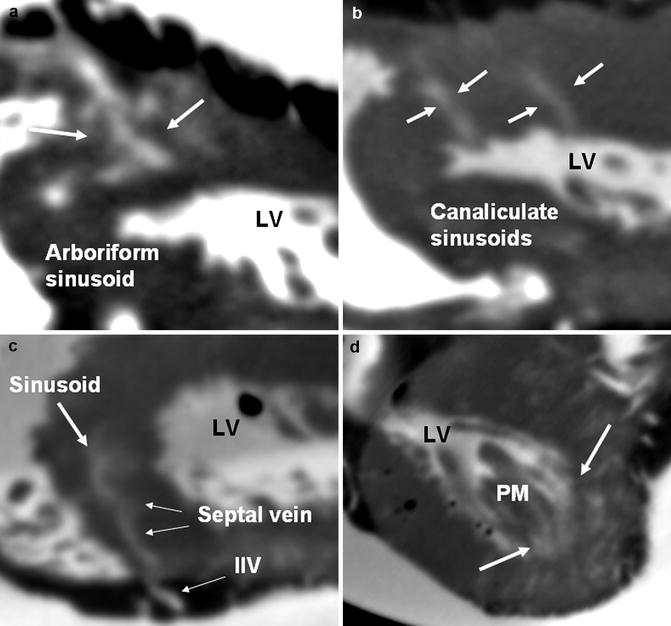
Fig. 28.3
(a) Schematic drawing demonstrates extensive interconnection of the epicardial cardiac vessels through the intraluminal Smaller-Cardiac Venous System (CVS). (b) Tributaries of the Smaller-CVS (Thebesian vessels): 1. Venoluminal vessels connect intramural venules with the lumen of cardiac chambers. 2. Venosinusoidal vessels connect intramural venules with subendocardial sinusoids and then the lumen. 3. Arterioluminal vessels connect arterioles with the atria or ventricles without traversing capillary beds. Only exist in the right ventricle (RV). 4. Arteriosinusoidal vessels connect arterioles with sinusoidal spaces. RA right atrium, LV left ventricle, LA left atrium
Fig. 28.4
Short-axis CT images of the heart showing large sinusoids in the interventricular septum and an example of myocardial cleft of the interventricular septum. Clefts should not be mistaken with a ventricular septal defect RV right ventricle, LV left ventricle
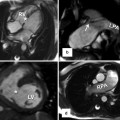
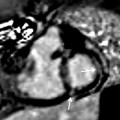
Fig. 28.5
Ex vivo CT of the heart in different specimens. The coronary veins are opacified with 10 % iodinated contrast injected into the coronary sinus. Note numerous contrast-filled intramural Thebesian vessels including sinusoids (thick white arrows) some opening into the ventricular lumen. Arboriform (a) and canaliculate (b) sinusoid morphologies are shown. (c) demonstrates a venosinusoidal communication connecting the inferior interventricular vein (IIV) with a sinusoid through the septal vein. (d) Shows large sinusoids at the base of left ventricle (LV) papillary muscle (PM). Thebesian vessel foramina are common at the apex of the ventricles and at the base of the papillary muscles
The vessels of the Smaller-CVS are collectively called Thebesian veins. However, in view of their arterial component, the term “Thebesian vessels” is preferred [6]. Four distinct parts are described (Fig. 28.3b). Their orifices are found in cardiac chambers (mostly RA and right ventricle) and bases of papillary muscles [9, 10] and usually are <0.5 mm in diameter but can be much larger especially in congenital heart disease with abnormal drainage of the CS [11]. Approximately 70–80 % of the left coronary artery blood flow drains through the CS tributaries, and the remainder is drained via the Smaller-CVS [12–15]. The right heart chambers mainly drain thorough the Smaller-CVS [6, 8]. In patients with single ventricle and atrial isomerism, this drainage pattern may be different due to rearrangement of the epicardial veins. The Thebesian network can provide reverse flow from ventricles into the epicardial coronary arteries when flow in the latter is compromised [12]. In patients with congestive heart failure, congestion is mainly in large veins not the Thebesian veins [13]. Enlarged Thebesian veins are described in CHD patients.
Atrial Venous System
Imaging of these veins is difficult because of small size of vessels. However careful evaluation of cardiac CT images can show these structures in many studies. Different classifications are introduced [6, 8, 16, 17]. The easiest classification is introduced by von Lüdinghausen [8] (Table 28.1).
Table 28.1
Venous drainage of the left and right atrial walls
Left atrium | Right atrium |
|---|---|
1. Posterior and lateral walls (99 %) | 1. Small intramural veins (73 %) |
Draining into the CS | Draining into the RA, 1 mm diameter |
2. Septal walls | 2. Venous tunnels of the RA (right atrial CS) (25–60 %) |
Draining into the RA (92 %) | 1–12 cm in length and 1–4 mm in diameter – emptying into the RA or SCV |
Anterosuperior (near SVC) (99 %) | 3. SAN region |
Posteroinferior (near IVC) (35 %) | Small veins and sinusoids draining into the RA |
3. Posterosuperior wall | 4. AVN region |
Draining into the mediastinal veins (40 %) | Small venous tunnels draining into the RA or CS |
Directly draining in the LA (80 %) | |
Draining into the pulmonary veins (some) |
Veins of the LA Wall
The majority of left atrial veins are tributaries of the Greater-CVS. Three groups are described [6, 8]:
1.
Veins of the posterior and lateral walls of the LA empty into the CS and GCV (Fig. 28.6).
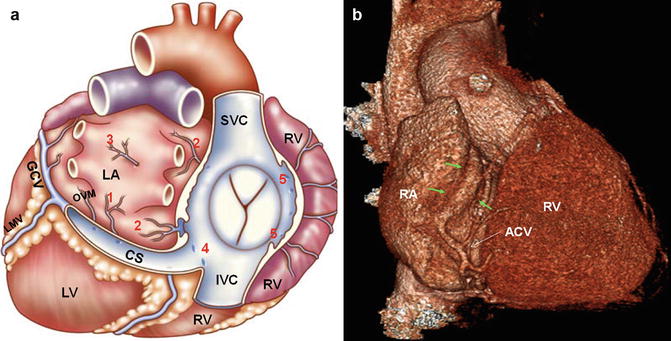
Fig. 28.6
(a) Atrial venous system. Posterosuperior view of the heart is depicted. The right atrium is removed. 1. Veins of the posterior and lateral walls of the left atrium (LA) empty into the coronary sinus (CS). 2. Septal veins of the LA drain into the right atrium (RA). 3. Posterosuperior wall of the LA drains into the LA lumen or the superior pulmonary veins. 4. Atrioventricular node region contains small sinusoids draining into the RA near the CS ostium. 5. Anterior cardiac veins may drain directly into the RA, small cardiac vein, or into a venous tunnel in the RA wall. (b) Drainage of the anterior cardiac vein (ACV) into the venous tunnel running (green arrows) parallel to the atrioventricular groove. LV left ventricle, RV right ventricle, SVC superior vena cava, IVC inferior vena cava, OVM oblique vein of Marshall, LMV left marginal vein, GCV great cardiac vein
2.
Septal veins of the LA drain into the RA through the interatrial septum. These veins are commonly seen with CTA. Veins anterosuperior to the fossa ovalis pass through the interatrial groove and empty in to right atrium near the superior cavoatrial junction (Fig. 28.7). Some (12 %) may pass through superior interatrial muscle connections where Bachmann bundle is located [18] (Fig. 28.8). Enlargement of these veins can rarely occur in arteriovenous malformations of the atrial vessels (Fig. 28.9). Veins inferoposterior to fossa ovalis are less common (Fig. 28.7).
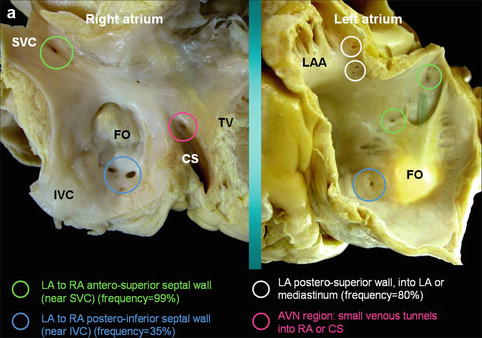
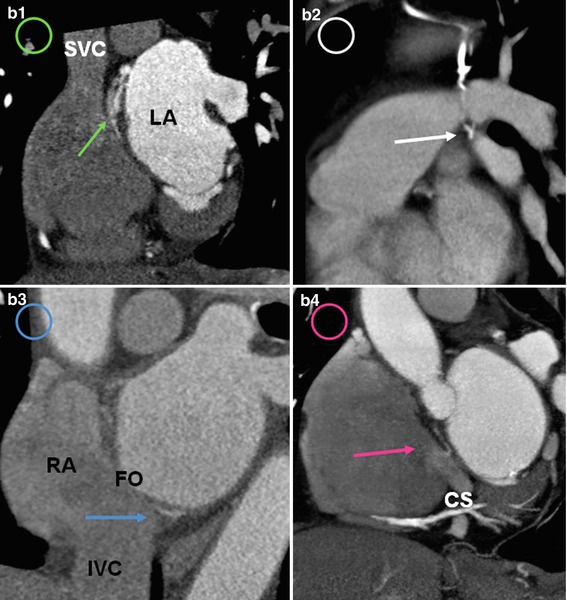
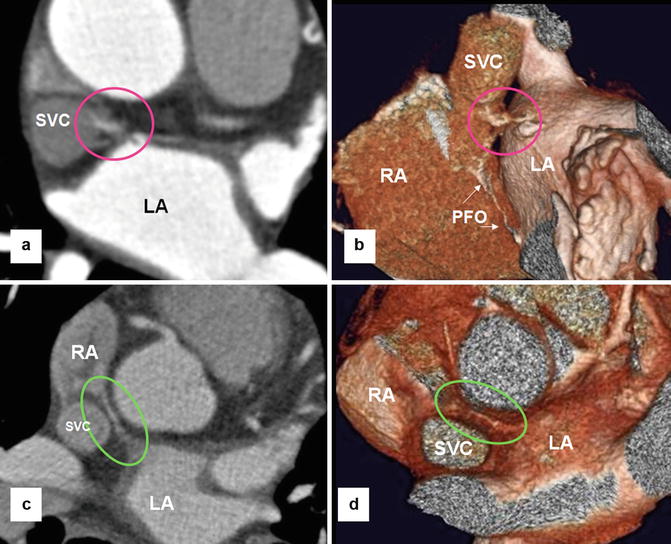
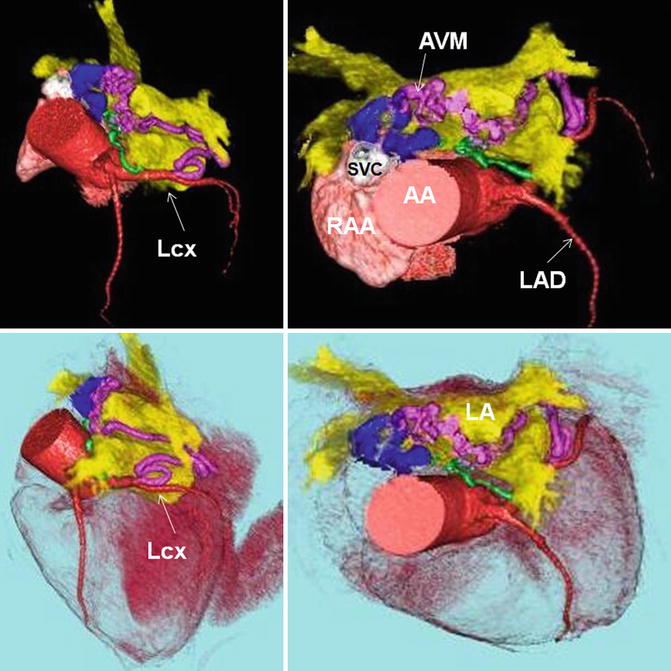
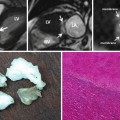
Fig. 28.7
(a) Septal views of the right and left atria (RA, LA) from two different cadaveric specimens are shown. Most of the septal venous drainage occurs from the LA into the RA. Venous drainage of the anterosuperior and posterosuperior of the interatrial septum as well as posterosuperior wall of LA and atrioventricular node (AVN) region is shown by green, blue, white, and pink circles, respectively. Most of the septal venous drainage occurs from the LA into the RA. The venous opening can be large enough to be detected by CT scan. (b) Short-axis CT images demonstrate the drainage pattern of atrial wall veins matching to the colored circles shown in (a) including communication between the two atrial walls near the SVC (green arrow in b1) and IVC (blue arrow in b3), the superior wall of the LA near confluence with left superior pulmonary vein (white arrow in b2), and the medial RA wall near the coronary sinus (CS) ostium (pink arrow in b4). Veins of the superior wall of LA may communicate with venous collaterals in the mediastinum (white arrow in b2). LAA left atrial appendage, FO fossa ovalis, SVC superior vena cava, IVC inferior vena cava, TV tricuspid valve
Fig. 28.8
Venous drainage of the anterosuperior septal wall of left atrium (LA) into the right atrium (RA) through the superior interatrial muscle connection where Bachmann bundle resides. Communications found in two different patients are shown by pink (a, b) and green (c, d) circles. This communication is seen in 12 % of CT angiographies. The lumen of a patent foramen ovalis (PFO) is incidentally seen (white arrows). SVC superior vena cava
Fig. 28.9
Color-coded CT angiography shows arteriovenous malformation (AVM) in the transverse sinus near the superior cavoatrial junction. Arterial supply is provided by an atrial branch (in green) and the left sinoatrial node (in pink) arteries both arising from the left circumflex (LCx) artery. Enlarged draining atrial veins (blue) are seen near the junction of the superior vena cava (SVC) with the atrium. Left atrium (LA) is shown in yellow. AA ascending aorta, RAA right atrial appendage, LAD left anterior descending artery
3.
Posterosuperior wall of the LA near the left atrial appendage drain into the LA and superior pulmonary veins (Fig. 28.7). They may connect to the mediastinal veins, azygos or hemiazygos venous system, and bronchial veins [8]. The mediastinal connections can be important alternative route for venous return to the atria incase of occlusion of pulmonary, brachiocephalic, or superior vena cava occlusion (Figs. 28.7 and 28.8). In congenital atresia of the CS, the myocardial venous drainage can be via ectatic atrial veins of the LA [19].
Veins of the RA Wall
The majority of the right atrial wall veins are located intramurally and drain into the RA. The veins draining the wall of the right atrial appendage have no connection with the epicardial veins and therefore are classified as Smaller-CVS. The RA veins are classified into four groups based on anatomical locations (Table 28.1).
1.
Small intramural venous tunnels draining directly into the RA: They are a few mm in length and 1 mm diameter [6].
2.
Venous tunnels of the RA: Termination of the anterior cardiac veins of the right ventricle is variable. They may drain directly into the RA, small cardiac vein, or in some into a venous tunnel [6]. When it exists, this venous tunnel runs parallel and 1–2 cm above to the tricuspid orifice along the posterior or posterolateral wall of the RA [20] (Fig. 28.6). In high-quality CTAs, these veins may be partially visible (Fig. 28.6b). This system of drainage was initially described as “the small cardiac vein.” This SCV can drain either separately into the right atrium or into the CS.
3.
Sinoatrial node region: The sinoatrial node region has sinusoids draining into the RA [14]. This network of anastomosing blood vessels theoretically can protect the node in case arterial supply is compromised. However, this phenomenon is rare given the common variants of dual or multiple arterial supplies to the node.
4.
Atrioventricular node region: Venous tunnels are seen at the base of interatrial septum near the atrioventricular node and His bundle and usually open into the RA near the ostium of the CS or directly into the CS (Figs. 28.6 and 28.8). These tunnels can be seen in CTA and should not be confused with anomalous vessels or a patent foramen ovale.
Anterior Right Ventricular Venous System
Including the anterior cardiac, right marginal and conus veins are present in 90 % of cases [6, 20–22] (Table 28.2).
Table 28.2
Characteristics of the epicardial veins of coronary sinus and anterior right ventricle venous system
Veins | Origin | Territory | Ostial diameter (mm) | Frequency % | Drainage | Number | Variant | Ostial valve % |
|---|---|---|---|---|---|---|---|---|
CS | GCV | Left atrioventricular groove | 4–14 (10) | 99 | RA | 1, duplication is very rare | Absence (with left SVC), unroofed, atresia (1 %), duplication | 80 |
GCV/AIV | Apex | Anterior septum, anterior of both ventricles, parts of LA and apex | AIV = 09–4.4 (2.7), GCV = 1.2–6.3(3.9) | 100 | CS (99 %) | 1(98 %) | Aberrant course to RA in 1 %, aneurysm, myocardial bridge 2–8 %, duplication 3 %, myocardial belt (6 %) | 85 |
IIV | Apex | Posterior wall of the RV and LV, apex, posterior two third of the interventricular septum | 2–5.3 (3.6 ) | 100 | CS, rarely RA (2.5 %) | 1 (75 %), 2 (24 %) | Aneurysm (8 %), varicoid, duplicated, myocardial cover (2.5 %) | 60 |
LPV | Posterior wall | Lateral and diaphragmatic walls of the LV | 1–5.5 (2.4) | 95 | CS (37–77 %), GCV (13 %) | 1 (63 %), 2 (23 %), multiple small (9 %), non (5 %) | Bulbar (5 %), myocardial cover (2 %) | 30 |
LMV | Posterolateral wall of LV | Draining much of LV myocardium | 1–3 (2.2) | 70–85 | GCV (80 %), CS (20 %) | 1 | Absence common | 30 |
SCV | Right atrioventricular groove | Diaphragmatic surface of RV | <1 | 30–50 | CS (85 %), IIV (12 %) | 1 | Can receive the right marginal vein in 10 % | – |
OVM | Junction of CS and GCV | Posterolateral LA, 2–3 cm length | 0.4–1.8 | 85–95 | CS | 1 | Persistent SVC 0.5 % | – |
RMV | Apex | Anterior and posterior RV walls | 0.5–3 | 13–80 | SCV (30 %), rest RA or tunnel of RA | 1 | Large draining into a vertical RA tunnel | – |
ACV | Anterior RV | Anterior and anterolateral RV | 0.5–1 | 90 | RA (30 %), venous tunnel of RA (66 %), SCV | 1 (24–57 %), 2(33–48 %), 3(9–28 %), up to 15 tiny ones | Abnormal course of AIV into SVC, large conus vein | 12 |
The anterior cardiac veins drain 2/3 of the right ventricle including the anterior and anterolateral walls of the right ventricle. These veins are frequently identified in coronary CTAs (Fig. 28.10). They are variable in sizes and numbers and usually drain into the RA just above the atrioventricular groove [6, 16, 21]. In 5–27 % they merge to form a common trunk before entering the RA [6, 21].
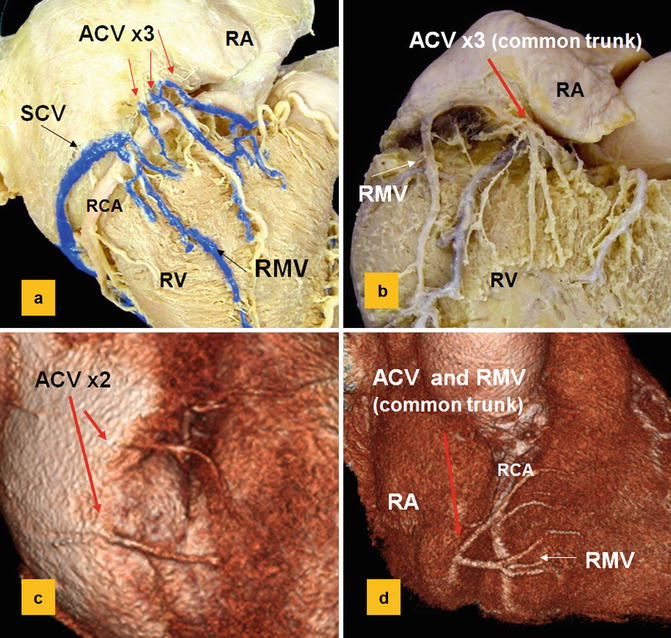
Fig. 28.10
Common variants of the right ventricle (RV) venous system are shown: cadaveric specimens (a, b) and CT angiograms (c, d). Passing anterior to the right coronary artery (RCA), the anterior cardiac veins (ACV) commonly enter into right atrium (RA) as separate vessels or in some cases form a common trunk (5–27 %). The right marginal vein (RMV) is seen in 80 % of cases. It drains in to small cardiac vein (SCV) in 30 % or drains directly into the RA in 70 %
The right marginal vein originates near the right ventricular apex and receives branches from posterior and anterior surfaces of the right ventricle (Fig. 28.10). In one third the vein continues as small cardiac vein into the CS [6]. In the remainder of cases, it drains into the RA or the venous tunnels of the RA.
The conus (infundibular) veins are usually small veins and drain into the RA. However, they can be large and varicoid creating diagnostic problems (Fig. 28.11) or causing excessive bleeding during surgery. Veins of Zuckerkandl and Cruveilhier are described in anatomic literature for veins draining the anterior or posterior surfaces of the infundibulum, respectively [20, 21] (Fig. 28.11).
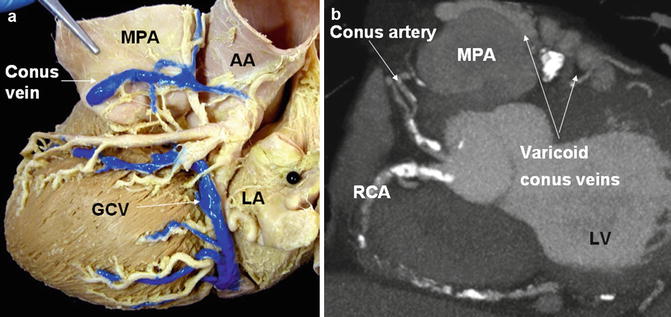
Fig. 28.11
Conus veins. (a) In this cadaveric specimen the conus vein is the vein located between the main pulmonary artery (MPA) and the ascending aorta (AA). Large and varicoid conus veins are seen in coronary artery occlusions, myocardial bridging, and vascular malformations. (b) Dilated conus vein is shown in a patient with severe coronary artery disease and right coronary artery (RCA) occlusion, (GCV) great cardiac vein, (LA) left atrium, (MPA) main pulmonary artery, (LV) left ventricle
Coronary Sinus Tributaries
The coronary sinus tributaries include the CS, the GCV, the left marginal vein, the posterolateral vein of the LV, and the inferior interventricular vein (IIV) (Fig. 28.12). In 30 % it receives the right marginal vein blood through the small cardiac vein [6] (Table 28.2).
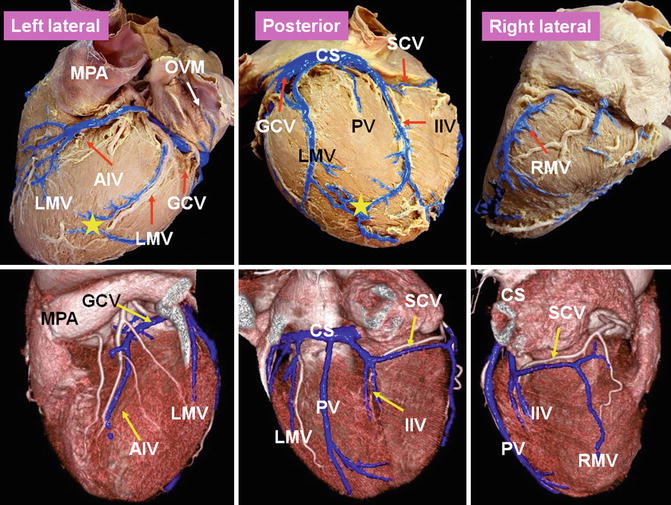
Fig. 28.12
Left lateral, posterior, and right lateral views of the cadaveric heart (upper row) and CT angiographies of a patient with tetralogy of Fallot (lower row). Tributaries of the coronary sinus (CS) venous system are displayed in blue. The CS tributaries include the CS, the great cardiac vein (GCV), the anterior interventricular vein (AIV) portion of the GCV, the left marginal vein (LMV), the posterior vein (PV) of the left ventricle, the inferior interventricular vein (IIV), the oblique vein of Marshall (OVM), and the small cardiac vein (SCM). A very large PV and two small IIVs are shown (yellow asterisks) in CT image of patient with tetralogy of Fallot. In cadaveric heart the right marginal vein (RMV) drains directly into the right atrium, while in tetralogy case, it is draining into the SCV. That is why SCV is large in this patient; it also drains into the IIV. MPA main pulmonary artery
Imaging Methods
The CS is frequently used as a conduit for catheter treatment of arrhythmias as well as left ventricular pacing. These procedures are well known for their potential technical difficulties. As a result different imaging methods are introduced for evaluation of this system. Each technique has its own advantages and limitations [23–29].
Retrograde venography via the CS is currently the standard technique for defining the CS anatomy; however, it is invasive in nature and can be technically challenging. This technique is frequently used to show the anatomy of the CS and target veins for CRT. In this technique using an occlusive balloon contrast in injected into the CS and two orthogonal views including right anterior oblique 45° and left anterior oblique 45° are obtained [23]. High-speed rotational coronary venography uses rapid isocentric rotation over a 110° arc in 4 s, acquiring 120 frames/angiogram [23]. With this modification, vessel overlap and foreshortening will be reduced, and target veins including second-degree tributaries can be better defined. Levophase of coronary angiography is preferred by some investigators and claimed to better define the anterior interventricular vein (AIV) and IIV as well as the peripheral branches compared to retrograde venography [24]. However, the sensibility of this method is questionable. The technique takes advantage of the coronary artery angiography procedure commonly indicated in the assessment of candidates for CRT.
MRI and CT have been increasingly used to assess anatomy of the coronary vessels including coronary veins [25–29]. CT has the advantage of showing part of the CS and in some cases the confluence of the IIV which may be obscured with balloon in retrograde venography. With CT there is no foreshortening or vessel overlap. CT also demonstrates many ancillary structures such as coronary arteries, old infarctions, interatrial septum anatomy, and variants of the normal anatomy. Higher radiation dose in CT is a limitation [26] which can be modified using dose reduction techniques. CT also may have difficulty showing second-order tributaries of the coronary veins in routine coronary CTAs. Demonstration of the oblique vein of left atrium is also more challenging with CT compared with retrograde venography. However, with some modification of the CT technique, most small branches can be nicely depicted. CT technique for cardiac venous mapping is very similar to routine coronary CTA [18]. For optimal visualization of the coronary venous system, the trigger delay for data acquisition should be delayed 2–3 s to let the coronary venous side fill with contrast. This can easily be achieved with selecting the automated trigger level in the descending aorta approximately 3 cm below the tracheal bifurcation and starting scan 4 s after reaching a threshold of 180 Hounsfield units (HU).
Great Cardiac Vein
The GCV is the longest and the most consistent vessels making up the cardiac venous system almost always enters the CS [30–34]. This vein drains blood from the anterior interventricular septum, the anterior surfaces of both ventricles, part of the LA, and the apical region of the heart [6




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
