I. Global or regional dysfunction and structural alterations
Major criteria by MRI:
Regional RV akinesia, dyskinesia, or dyssynchronous RV contraction and 1 of the following:
Ratio of RV end-diastolic volume to BSA ≥110 mL/m2 (male) or ≥100 mL/m2 (female)
Or RV ejection fraction ≤40 %
Minor criteria by MRI:
Regional RV akinesia, dyskinesia, or dyssynchronous RV contraction and 1 of the following:
Ratio of RV end-diastolic volume to BSA ≥100 to <110 mL/m2 (male) or ≥90 to <100 mL/m2 (female)
Or RV ejection fraction >40 to ≤45 %
II. Tissue characterization of wall
Fibrous replacement of the RV free wall myocardium in ≥1 sample, with or without fatty replacement of tissue on endomyocardial biopsy, plus one of the following major or minor criteria:
Major criteria: Residual myocytes <60 % by morphometric analysis (or <50 % if estimated)
Minor criteria: Residual myocytes 60–75 % by morphometric analysis (or 50–65 % if estimated)
III. Repolarization abnormalities
IV. Depolarization/conduction abnormalities
V. Arrhythmias
VI. Family history
Histologic Features
The primary histologic feature of ARVC/D is segmental or diffuse transmural loss of the RV free wall myocardium and its replacement by fibrofatty tissue. Fibrofatty replacement occurs as a wave-front phenomenon that extends from the epicardium toward the endocardium (Fig. 17.1) [13]. One revised criterion involves fibrous replacement of the myocardium with or without fatty replacement of the tissue at endomyocardial biopsy and calls for quantification of residual monocytes to determine whether this is a major or minor diagnostic consideration (Table 17.1) [5].
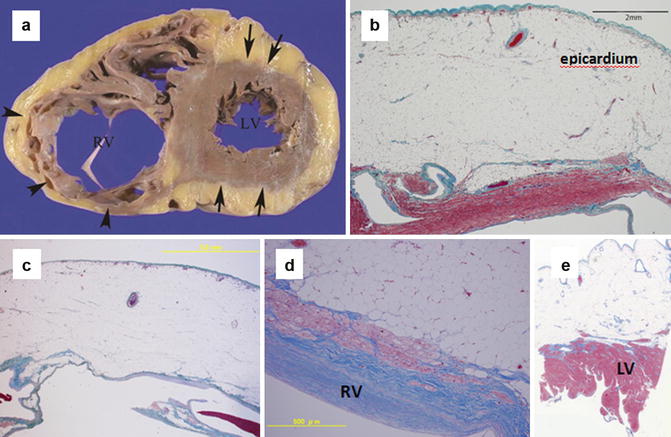
Fig. 17.1
Autopsy specimen of ARVC/D in a 67- year-old man who died of congestive heart failure. (a) Photograph of the cut surface of the heart shows marked thinning of the right ventricle (RV) free wall (arrowheads) with left ventricle (LV) involvement. (b, c) Low and (d) high power photomicrographs (Masson trichrome stain) of the RV lateral wall show fibrofatty myocardial replacement extending from the epicardium toward the endocardium. (c) Shows almost complete fibrofatty replacement of the RV myocardium. (e) Low power photomicrograph (Masson trichrome stain) also shows fibrofatty replacement from the epicardial side of the LV wall (From Kimura et al. [4] with permission)
The myocardium is commonly affected in the so-called triangle of dysplasia, which includes the outflow tract, inflow tract (inferior wall beneath the posterior leaflet of the tricuspid valve), and apex of the RV [5]. The RV free wall becomes thin and translucent in response to myocardial loss and fibrofatty replacement (Fig. 17.1). Nearly half of cases demonstrate saccular aneurysms at the apex and inferior wall of the RV [13, 14]. Histologic changes in the LV wall consist of transmural or predominantly subepicardial and mid-wall fibrofatty replacement that affects both the interventricular septum and the LV free wall either diffusely or, more often, regionally (Fig. 17.1). The wave front of the fibrofatty infiltration appears to extend from the outer to the inner layer of the LV wall, resembling the pattern of involvement of the RV free wall [15].
Imaging Findings
MR imaging findings are useful in diagnosing ARVC/D, and characteristic findings include dilatation of the RV, especially the RV outflow tract (RVOT) and part of the triangle of dysplasia in association with reduced RVEF and regional RV akinesia, dyskinesia, or aneurysm. Intramyocardial fat infiltration and thinning of the RV wall are common and usually coexist. Post-contrast images may show LGE of the RV free wall, ventricular septum, and/or LV free wall that suggests myocardial fibrosis [4–6, 8–10, 16] (Figs. 17.2, 17.3, and 17.4).
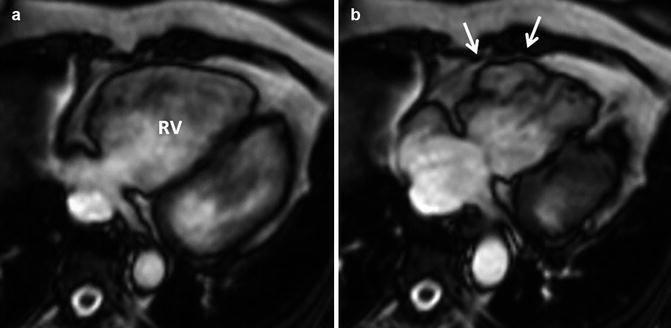
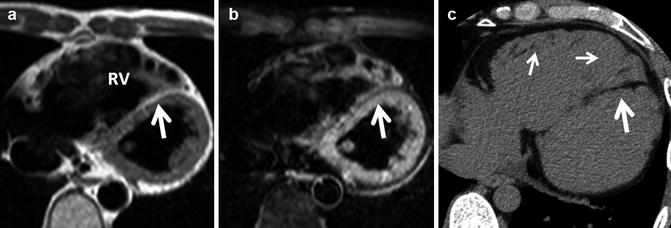
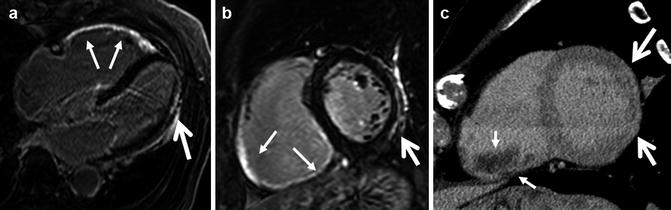
Fig. 17.2
ARVC/D according to the 2010 International Task Force criteria in a 50-year-old woman referred for evaluation of non-sustained ventricular tachycardia on Holter ECG. Cine MR imaging (a diastolic phase; b systolic phase) reveals systolic outpunching (dyskinesia) of the anterior wall of the RV (arrows)
Fig. 17.3
ARVC/D according to the 2010 International Task Force criteria in a 41-year-old man referred for evaluation of congestive heart failure. Black blood MR images without (a) and with (b) fat suppression show dilatation of the right ventricle (RV) with a thin RV free wall and myocardial fat in the ventricular septum (arrows). Small amounts of fat in the RV trabeculae demonstrated on noncontrast CT (c) are difficult to discern on MR imaging (small arrows). CT also shows extensive fatty infiltration of the interventricular septum (large arrow) (From Kimura et al. [4] with permission)
Fig. 17.4
ARVC/D according to the 2010 International Task Force criteria in a 78-year-old man referred for evaluation of syncope and non-sustained ventricular tachycardia on Holter ECG. MR images of 4-chamber (a) and short-axis (b) views show distinct LGE in the RV anterior and inferior walls (thin arrows) and the LV lateral wall (thick arrow). A delayed post-contrast short-axis CT image (c) also shows late enhancement of the LV lateral wall (large arrows), which is less distinct than the MR image. CT does not demonstrate the region of late enhancement of the RV wall. Thrombus is seen in the RV cavity (small arrows) (From Kimura and Nakajima [17] with permission)
Cine MR imaging is widely used to measure RV size and EF and evaluate wall motion abnormality (Fig. 17.2). It enables diagnosis of early and subtle cases of ARVC/D by detecting regional wall motion abnormality, which is thought to precede global and systolic dysfunction during disease progression. Aneurysm of the RV free wall is also a characteristic finding on cine MR imaging, appearing as a focal outpouching of the wall. The revised criteria include qualitative and quantitative MR findings to diagnose global or regional dysfunction and structural alterations; ARVC/D diagnosis requires a combination of RV dilatation or reduced RVEF and regional wall motion abnormalities [5] (Table 17.1).
It is important to know that the presence of RV myocardial fat is not specific to ARVC/D (Fig. 17.3) and appears to be but a common finding in elderly individuals and also in the scars of myocardium of patients with other cardiomyopathies [4]. Moreover, MR findings suggesting RV myocardial fat (high signal intensities on fast spin echo sequence) are least reproducible because of the thin RV myocardium and various artifacts related primarily to blood flow. Therefore, the Task Force does not include MR evidence of RV myocardial fat in its diagnostic criteria for ARVC/D.
MR imaging with LGE is a well-established mean of detecting myocardial fibrosis, but MR findings of myocardial fibrosis of the RV free wall (LGE) are not among the revised criteria, probably because of the limited spatial resolution of MR for detection of LGE in a thinned wall RV and scarce literature support on the utility of LGE for diagnosis of ARVC/D. We have found LGE with fat suppression and thin slice thickness (5 mm) useful in detecting myocardial fibrosis of the RV free wall (Fig. 17.4). Myocardial fibrosis (LV involvement) of the thicker LV wall is well demonstrated with LGE. LGE is most frequently seen in the subepicardial layer followed by the midwall of the LV myocardium. The anatomical locations of LGE in descending order are inferolateral wall, inferior wall-septal junction, inferior wall, septum, anterolateral wall, and anterior wall (Fig. 17.4) [8]. These anatomic distributions of LGEs correlate well with pathologic reports of ARVC/D [15].
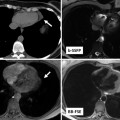
CT images are useful in diagnosing ARVC/D, especially in patients with implantable cardioverter defibrillator. Although CT is not included in either the original or revised criteria, ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac CT recognized the utility of CT in assessing RV morphology and patients with suspected ARVC/D [18]. Several characteristic CT findings of ARVC/D are reported including dilatation of the RV including outflow tract, thin RV free wall, myocardial fat in the RV trabeculae and moderator band, conspicuous trabeculae, and scalloped or bulging appearance of the RV free wall [4, 19] (Figs. 17.5 and 17.6). In our experience with CT scan in ARVC/D patients, the RV free wall is usually imperceptibly thin as a result of fibrofatty replacement extending from the epicardium toward the endocardium. On CT, fat is frequently seen in the ventricular septum, especially in the RV side of septum, and the LV involvement usually appears as areas of wedge-shaped or band-like fat deposition in the subepicardial LV free wall [4] (Figs. 17.5 and 17.6). Myocardial fat and wall thinning are more easily and precisely recognized with CT than MR imaging. The lower contrast resolution of CT compared with MR imaging limits its utility in detecting myocardial fibrosis using delayed enhancement (Fig. 17.4).

Get Clinical Tree app for offline access
Fig. 17.5
Histologically proved ARVC/D in a 67-year-old man who died of congestive heart failure (same patient as in Fig. 17.1). Axial pre-contrast (a




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
