Fig. 17.1
Atrial septal defect. Four-chamber CT image shows a large secundum atrial septal defect (asterisk) between the right atrium (RA) and the left atrium (LA) (a). An extracardiac conduit (arrow) of Fontan operation is noted. En face view reveals the size and shape of the atrial septal defect (asterisk) (b)
17.5.2 Ventricular Septal Defect
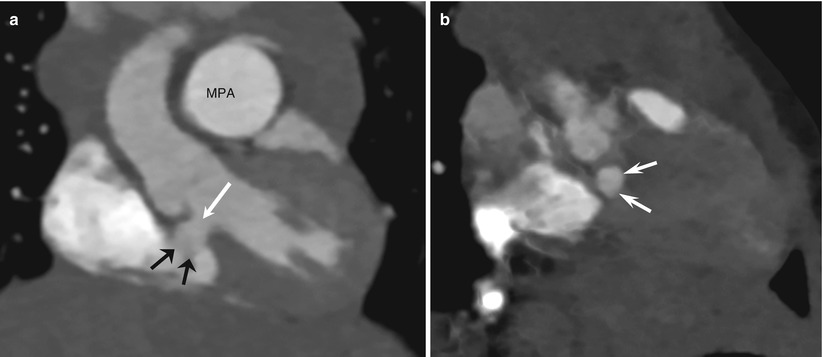
Fig. 17.2
Ventricular septal defect. Coronal CT image demonstrates a perimembranous ventricular septal defect (long arrow) with septal aneurysm (short arrows) (a). The dilated main pulmonary artery (MPA) is noted. En face view shows the size and location of the ventricular septal defect (arrows) (b)
17.5.3 Tetralogy of Fallot
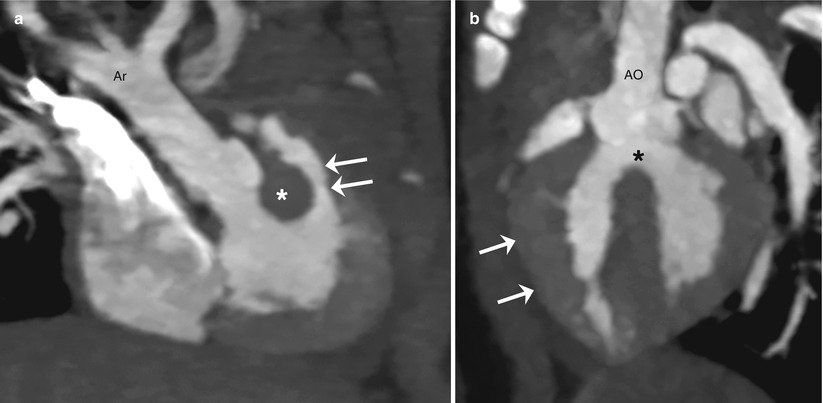
Fig. 17.3
Tetralogy of Fallot. Oblique coronal CT image shows an infundibular narrowing (arrows) and the stout outlet septum (asterisk) (a). The right aortic arch (Ar) is noted. Oblique sagittal CT image demonstrates a ventricular septal defect (asterisk) and overriding of the aorta (AO) (b). The right ventricular hypertrophy (arrows) is noted
17.5.4 Atrioventricular Septal Defect
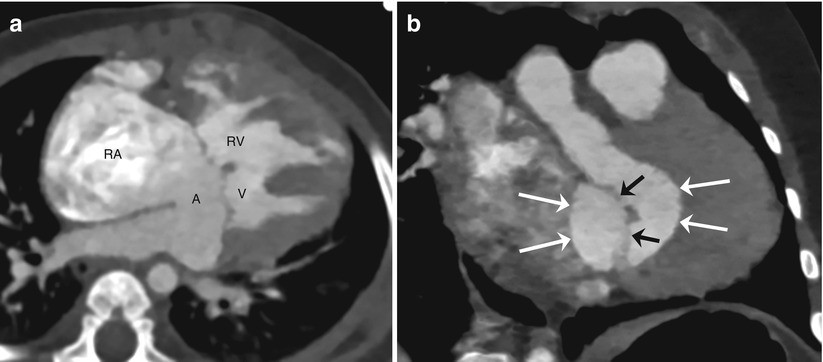
Fig. 17.4
Atrioventricular septal defect. Four-chamber CT image shows an atrioventricular septal defect consisted of a primum atrial septal defect (A) and an inlet ventricular septal defect (V) (a). The right atrium (RA) and the right ventricle (RV) are enlarged. The right ventricular hypertrophy is also noted. En face view reveals the size and shape of the defect (long arrows) (b). The atrioventricular valve (short arrows) is noted
17.5.5 Pulmonary Atresia
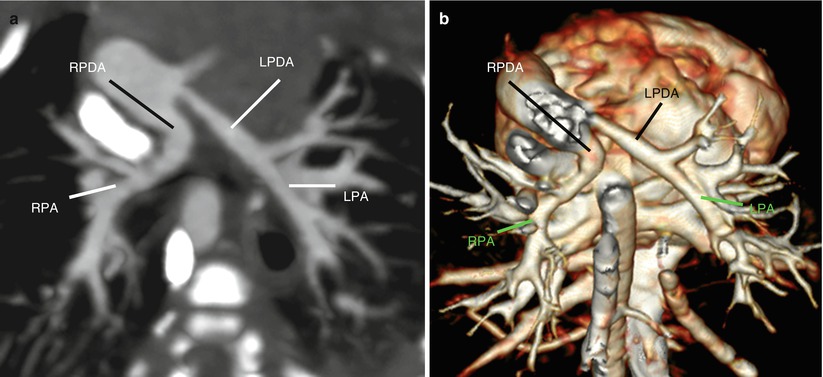
Fig. 17.5
Pulmonary atresia with non-confluent central pulmonary arteries. Oblique axial CT image (a) and volume-rendered CT image (b) demonstrate that the right (RPA) and left (LPA) pulmonary arteries are supplied from the right (RPDA) and left (LPDA) patent ductus arteriosi, respectively
17.5.6 Transposition of the Great Arteries
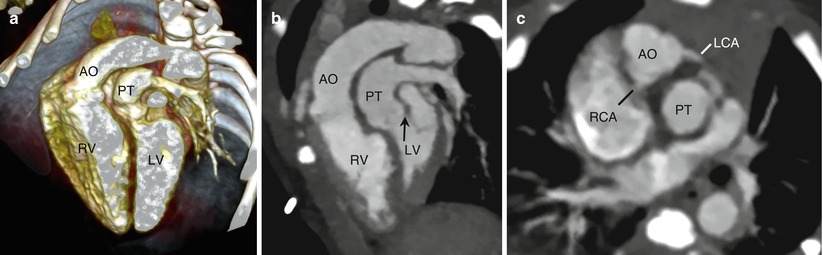
Fig. 17.6
Transposition of the great arteries. Volume-rendered CT image (a) and reformatted CT image (b) show that the ascending aorta (AO) arises from the morphologic right ventricle (RV) and the pulmonary trunk (PT) arises from the morphologic left ventricle (LV). The imaging finding is consistent with ventriculoarterial discordance. Pulmonary-mitral fibrous continuity (arrow) typical for transposition of the great arteries is noted (b). Oblique axial CT image demonstrates the malpositioned ascending aorta right and anterior to the pulmonary trunk that refers to d-malposition of the great arteries commonly seen in complete transposition of the great arteries (c). The origins of the right (RCA) and left (LCA) coronary arteries are also seen
17.5.7 Double Outlet Right Ventricle
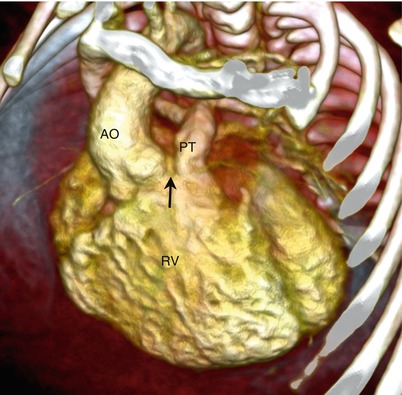
Fig. 17.7
Double outlet right ventricle. Volume-rendered CT image demonstrates that both the ascending aorta (AO) and the pulmonary trunk (PT) originate from the right ventricle (RV). Of note, the outlet septum is completely deficient (arrow)
17.5.8 Ebstein Anomaly
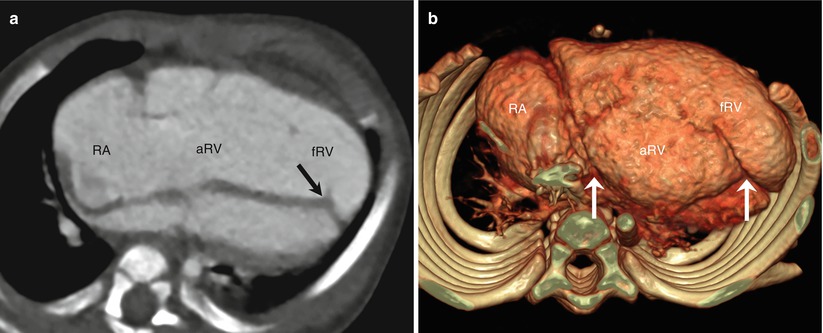
Fig. 17.8
Ebstein anomaly. Four-chamber CT image shows a diagnostic finding of the apically displaced septal attachment (arrow) of the tricuspid valve that divides the right ventricle into the atrialized (aRV) and functioning (fRV) portions of the right ventricle (a). The right atrium (RA) and the right ventricle are severely dilated. Inferior volume-rendered CT image reveals a characteristic trilobed appearance (arrows) consisting of the enlarged right atrium, the atrialized right ventricle, and the functioning right ventricle (b)
17.5.9 Tricuspid Atresia
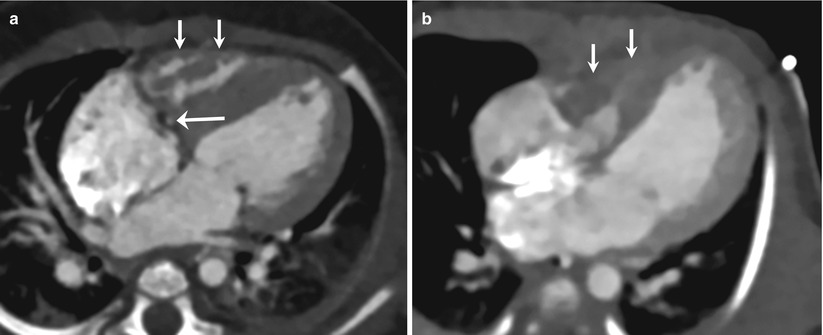
Fig. 17.9




Tricuspid atresia. Four-chamber CT image shows the absent right atrioventricular connection occupied by areolar sulcus tissue with the deeply invaginated right coronary artery (long arrow) (a). Four-chamber CT image demonstrates the rarer type of tricuspid atresia in which the tricuspid valve is present but atretic (b). In both cases (a, b), the right ventricle (short arrows) appears severely hypoplastic
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
