, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
Please refer to section “Airway Disease (Bronchiectasis and Bronchiolectasis)” in Chap. 13.
Definition
Please refer to section “Airway Disease (Bronchiectasis and Bronchiolectasis)” in Chap. 13.
Diseases Causing Bronchiectasis and Bronchiolectasis
Diffuse form of bronchiectasis occurs in variety of genetic abnormalities, especially those with abnormal mucociliary clearance or structural abnormalities of the bronchus or bronchial wall (cystic fibrosis [Fig. 25.1], dyskinetic cilia syndrome, Williams–Campbell syndrome). Nontuberculous mycobacterial disease is the most common infectious causes of diffuse bronchiectasis. Noninfectious causes include allergic bronchopulmonary aspergillosis and asthma. Also note section “Airway Disease (Bronchiectasis and Bronchiolectasis)” in Chap. 13.
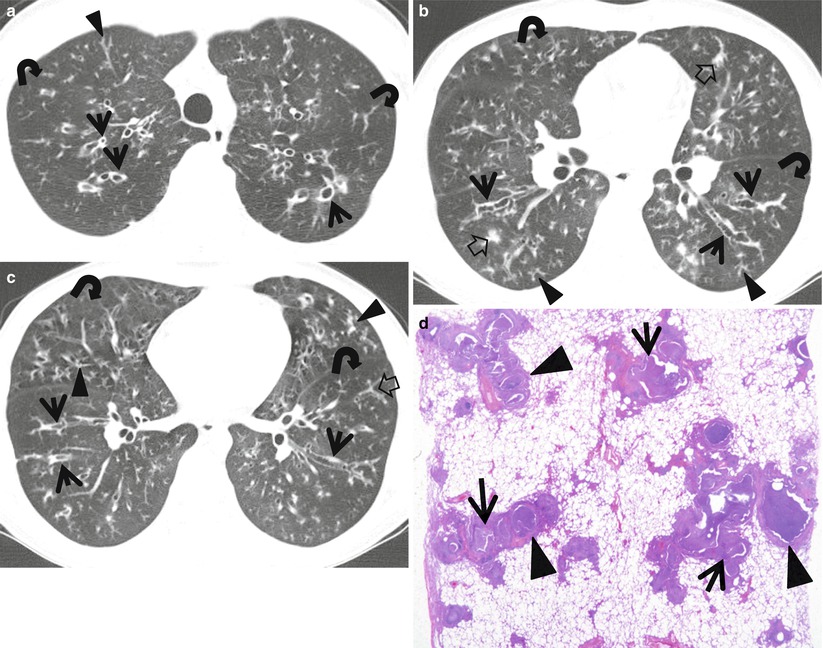
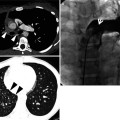
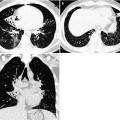
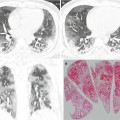
Fig. 25.1
Cystic fibrosis in a 23-year-old man. (a–c) Lung window images of CT scans (2.5-mm section thickness) obtained at levels of great vessels (a), lower lobar bronchi (b), and inferior pulmonary veins (c), respectively, show areas of bronchiectasis (arrows), tree-in-bud signs (arrowheads), and mucus plugging (open arrows). Also note mosaic perfusion areas (curved arrows). (d) Low-magnification (×4) photomicrograph of surgical biopsy specimen discloses bronchiolar dilatation (arrows) owing to luminal impaction of mucus and inflammatory exudates. Also note bronchiolar wall thickening (arrowheads) with chronic inflammation and fibrosis
Distribution
Please note section “Airway Disease (Bronchiectasis and Bronchiolectasis)” in Chap. 13.
Clinical Considerations
Please note section “Airway Disease (Bronchiectasis and Bronchiolectasis)” in Chap. 13.
Key Points for Differential Diagnosis
Diseases |
|---|