Abstract
The decision to provide circulatory support to newborn infants is predominantly based upon a reliance on blood pressure (BP) values, typically by targeting mean BP values, which serve as a surrogate of cardiovascular well-being. Despite significant advances in other areas of newborn care, very little has changed in our approach to this relatively unique phenomenon. This reliance on BP as a surrogate of cardiovascular well-being remains problematic on a number of levels. In this chapter we explore the problems with this approach and provide further insight into the complexities involved in newborn cardiovascular assessment at the bedside.
Keywords
cardiac output, hypotension, intraventricular hemorrhage, mean blood pressure, perfusion
- •
In the context of neonatal care, invasive or noninvasive measurement of blood pressure can be accomplished with acceptable precision.
- •
Gestational- and postnatal-age-dependent population-based normative blood pressure ranges are available. However, their usefulness in the assessment of hypotension, defined as a blood pressure value associated with low systemic and organ blood flow and inadequate tissue oxygen delivery requiring treatment, is limited.
- •
Definition of hypotension based on physiologic principles, such as maintenance of cerebral blood flow autoregulation, provides more insight into the individual patient’s ability to effectively compensate for decreases in tissue oxygen delivery, However, the need for complex hemodynamic monitoring and data acquisition systems required for this approach has so far limited its clinical usefulness.
- •
Due to our inability to accurately diagnose hypotension, data on the association between blood pressure and short- and long-term outcomes have remained difficult to interpret.
- •
Thorough bedside clinical assessment and the use of sophisticated hemodynamic monitoring and data acquisition systems hold the promise of defining the individual patient’s compensatory capacity to combat decreases of tissue oxygen delivery. These approaches also enable the accurate, real-time, and individual-patient–based diagnosis of hypotension as well as provide the opportunity to test and find the most appropriate therapeutic interventions.
Targeting blood pressure (BP) values, in particular the mean arterial BP, as a surrogate of cardiovascular well-being has been the norm in neonatal intensive care units (NICUs) across the world for the past 30 years. Despite significant advances in other areas of newborn care, little has changed in our approach to this problem. A number of recent surveys conducted in Europe, Canada, and Australia have highlighted the continued reliance of clinicians on such an approach.
The reliance on BP as a surrogate of cardiovascular well-being remains problematic on a number of levels. There are different methods of obtaining BP measurements; there are many different normative BP ranges; there is a poor relationship between BP values and end organ blood flow; and there is an inconsistency in the relationship between BP values and subsequent clinical outcomes. In this chapter, we will explore these areas in further detail and provide insight into the complexities involved in newborn cardiovascular assessment at the bedside. These are set out as follows:
- 1.
Measuring BP
- 2.
Normative BP Ranges
- 3.
Clinical Factors Affecting BP
- 4.
BP and Short- and Long-Term Outcomes
- 5.
Bedside Clinical Assessment and Hemodynamic Monitoring
Measuring Blood Pressure
There are two main methods of obtaining BP measurements in newborn infants, noninvasively or invasively. Both methods have their own inherent advantages and potential problems, but the standard of care for any sick newborn infant should be invasive BP monitoring where feasible. Detailed recent reviews of BP measurement and monitoring in the neonate are available.
The noninvasive method is based on oscillometry. Marey first described this method in 1876. When a limb was placed in a pressure chamber, the pressure in the chamber would fluctuate, and the magnitude of these fluctuations was dependent on the pressure contained within the chamber. The oscillometric method is based on the principal that blood moving through an artery creates oscillations/vibrations of the arterial vessel wall. Thus, application of external pressure via an inflated cuff placed on the limb will allow determination of “arterial” BP parameters. These oscillations are transmitted to the cuff, converted into an electrical signal by the transducer, and ultimately display systolic, mean, and diastolic noninvasive BP measurements. Prior to the development of automated devices, values were obtained clinically by either palpation or auscultation. The palpation method relies on feeling a pulse, the auscultation method on listening for sounds of turbulence generated by flow in the partially compressed vessel. Korotkoff first described indirect measurements of BP by auscultation in 1905.
The systolic component of the BP measurement is just less than the systolic pressure at which the oscillations begin. The pressure at which the oscillations are at their maximum amplitude is the mean arterial pressure (MAP). The pressure in the cuff when blood first starts to flow continuously without vibration is an estimate of diastolic BP component. Various devices incorporate different algorithms to estimate the systolic and diastolic measurements.
There are a number of important factors that need to be considered when noninvasively measuring BP. Incorrect cuff size is the principal factor that will cause inaccurate measurements. The location of measurement, either an upper limb or a lower limb, may result in an overestimate or an underestimate of the true value, respectively. Also, different devices may result in slightly different readings related to the particular algorithm used. These will be discussed later.
The invasive method uses a fluid-filled transducer directly attached to an indwelling arterial catheter placed either in the aorta or in a peripheral artery. The pressure transducer converts the energy into an electrical signal that is then processed, amplified, and converted by a microprocessor into a visual display on the bedside monitor. There are a number of technical challenges that can result in inaccurate measurements, due to either overdamping or underdamping of the signal. One possible source of inaccuracy is the presence of small air bubbles introduced into the system. These can cause excessive damping of the pulse pressure waveform, causing an underreading of systolic BP and overreading of diastolic BP, although the mean BP is relatively unaffected. The absence or distortion of the dicrotic notch of the downward slope of the arterial waveform should suggest the presence of overdamping. Further sources of overdamping may occur if blood contaminates the tubing, if the tubing is too long or too compliant, or if the initial calibration process is inaccurate. Underdamping can occur with stiff noncompliant tubing or when there is hypothermia, characterized by excessively high systolic BP and low diastolic BP, as in a resonant signal.
A number of groups have compared different noninvasive devices and how they compare with invasive measurements. One of the author’s (ED) group has previously evaluated noninvasive measurements compared to invasive measurements with three different automated oscillometric devices: (1) Procare 300 Compact (Criticon Inc., Tampa, Florida), (2) GE Marquette Solar 8000 Patient Monitor (Fairfield, Connecticut), and (3) GE Dash 4000 Patient Monitor with DINAMAP technology (Fairfield, Connecticut). We also assessed the variability between simultaneously obtained upper and lower limb measurements. Measurement of the mid-arm and mid-calf circumference was obtained for each baby prior to placement of the appropriate-sized cuff (mid-arm and mid-calf circumference 0.45 to 0.55). This was consistent with the American Heart Association’s recommendation that the cuff bladder width and length be 40% and 80%, respectively, of the mid-arm circumference. Invasive measurements were recorded using a fluid coupled pressure transducer (Transtar R 19 Neonatal monitoring kit with Kids Kit Blood Sampling System; Medex Inc., Carlsbad, California). We found no significant difference between the noninvasive recordings simultaneously obtained from the upper or lower limbs. However, all three noninvasive recorders consistently overestimated invasive BP values. The average difference between mean invasive and noninvasive BP was 5.1 mm Hg overall and was device specific, 2.4, 4.5, 8.4 mm Hg for Dash, Dinamap, and Marquette monitors, respectively. These findings were similar to the findings of a number of other studies. Dannevig et al. found that Dinamap overreads mean BP by approximately 7.6 mm Hg, particularly in smaller infants. Diprose et al. also reported that Dinamap tends to overread mean BP in hypotensive infants—a finding subsequently confirmed by Chia et al.
The site at which the noninvasive recording is obtained may be one reason for this difference. A number of other studies comparing BP measurements from upper versus lower limbs have produced conflicting results. In term neonates, Park and Lee observed no difference in BP measurements between arm and calf measurements. Piazza and colleagues compared upper and lower limb systolic BP in term neonates in the first 24 hours and found that higher readings were generally present in the upper versus lower limb. However, higher readings in the lower limb were also common (28%). Cowan and colleagues determined arm and calf BP in term neonates in active and quiet sleep in the first 5 postnatal days. The increase in BP was greater in the arm than in the calf during these periods. Kunk and McCain studied 65 preterm neonates. They found no significant differences in systolic BP, diastolic BP, and mean BP between arm and calf values in the first 5 postnatal days, although arm BP values were consistently slightly higher. In summary, noninvasive BP measurements are device specific, and upper and lower limb mean BP values are similar, whereas noninvasive BP measurements tend to overestimate invasive BP values, particular in immature hypotensive preterm infants.
Blood Pressure Standards
Traditionally in medicine, treatment decisions are made when a particular parameter is outside a defined normative range. We believe these values represent levels that warrant intervention and are concerned that nonintervention might lead to an adverse outcome. Thus there is an accepted range above or below which intervention is warranted. However, in some areas of newborn care such clarity is often lacking. The management of hypoglycemia remains contentious. What is a low blood glucose level and its duration when one should worry? Is there a threshold level that warrants intervention? Similarly, BP ranges and management of low BP, primarily in preterm infants and especially during the transitional period, remain complex. When we investigate BP standards or normative ranges, the striking findings are first, the lack of consistency across these numerous ranges and second, the absolute number of ranges that exist. Ranges are often based on birth weight, gestational age, and postnatal age criteria. Similar populations of babies with different reference ranges suggest methodologic differences or problems. These statistically determined values vary considerably, which is not surprising considering how many of these ranges were derived. These include retrospective data collection; the inclusion of small numbers of patients; the collection of only a few data points and summation over wide time ranges; the combination of invasive and noninvasive measurements; and the inclusion of small for dates and appropriate for gestational age infants. In some instances, newborns who received volume or were on vasopressor-inotrope or inotrope infusions are included in normative range development. Thus it makes interpretation of these values challenging, as they are unlikely to constitute population-based “normative ranges.” However, they do provide very useful information to help inform clinicians at the bedside.
One of the first reference ranges developed was by Versmold et al. in 1981. Data were obtained invasively on 16 infants less than 1000 g and were subsequently combined with data from 45 larger infants to develop new nomograms for BP values during the first 12 postnatal hours in infants weighing 610 to 4220 g. The authors concluded that they “hope that the new, extended nomograms for mean, systolic, and diastolic blood pressures … will lead to more accurate assessment of the cardiovascular state in newborn infants, particularly in those born very prematurely.” It is now more than 30 years since this statement was written. Other reference ranges were developed in the 1980s and 1990s, including those from Watkins et al., Spinazzola et al., and Hegyi et al. While each study has some limitations, each provides important information. For example, Hegyi et al. highlight lower BP values in preterm infants receiving mechanical ventilation.
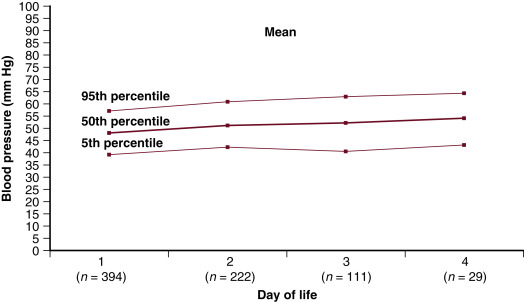
Kent et al. measured BP values in 406 healthy term infants on the postnatal ward over the first 4 postnatal days. The median systolic, diastolic, and mean BP values on the first postnatal day were 65, 45, and 48 mm Hg, respectively. On day 4, these values had increased to 70, 46, and 54 mm Hg. Fig. 3.1 depicts the mean BP values over the first days of postnatal life in well term newborns. These are useful reference guides when evaluating a term population of newborns. Kent and colleagues also evaluated noninvasive BP measurements in a group of stable preterm infants 28 to 36 weeks’ gestation. They measured BP on day 1, 2, 3, 4, 7, 14, 21, and 28 in a group of 147 infants. They found that premature neonates stabilize their mean BP after 14 days of postnatal life, and at this time they have a BP similar to that of term infants. Others have also shown an increase in BP over the first postnatal days. Watkins et al. document the mean and 10th percentile BP over the first days after delivery based on birth weight ( Table 3.1 ). Zubrow and colleagues reported the findings of a large multicenter study conducted by the Philadelphia Neonatal Blood Pressure Study Group. In this investigation, systolic and diastolic BP was significantly correlated with birth weight, gestational age, and postconceptional age. In each of four gestational age groups, systolic and diastolic BP was significantly correlated with postnatal age over the first 5 postnatal days. Batton and colleagues recently evaluated the change in BP over the first 24 hours after delivery in a population of extreme preterm infants. A drop in BP values characterized the first 4 postnatal hours. For the 164 untreated infants in this cohort, the systolic, diastolic, and mean arterial BP increased significantly ( P < .001) at an estimated mean ± SD rate of 0.3 ± 0.5 (range: −2.15 to 1.50), 0.2 ± 0.4 (range: −1.10 to 1.10), and 0.2 ± 0.4 (range: −0.90 to 1.25) mm Hg/h thereafter. This equates to an approximately 5 mm Hg increase in mean BP over the first 24 postnatal hours in preterm infants born less than 26 weeks’ gestation.
| Birth Weight (g) | Time (h) Postnatal Age | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 3 | 12 | 24 | 36 | 48 | 60 | 72 | 84 | 96 | |
| 500 | 35/23 | 36/24 | 37/25 | 38/26 | 39/28 | 41/29 | 42/30 | 43/31 | 44/33 |
| 600 | 35/24 | 36/25 | 37/26 | 39/27 | 40/28 | 41/29 | 42/31 | 44/32 | 45/33 |
| 700 | 36/24 | 37/25 | 38/26 | 39/28 | 42/29 | 42/30 | 43/31 | 44/32 | 45/34 |
| 800 | 36/25 | 37/26 | 39/27 | 40/28 | 41/29 | 42/31 | 44/32 | 45/33 | 46/34 |
| 900 | 37/25 | 38/26 | 39/27 | 40/29 | 42/30 | 43/31 | 44/32 | 45/34 | 47/35 |
| 1000 | 38/26 | 39/27 | 40/28 | 41/29 | 42/31 | 43/32 | 45/33 | 46/34 | 47/35 |
| 1100 | 38/27 | 39/27 | 40/29 | 42/30 | 43/31 | 44/32 | 45/34 | 46/35 | 48/36 |
| 1200 | 39/27 | 40/28 | 41/29 | 42/30 | 43/32 | 45/33 | 46/34 | 47/35 | 48/37 |
| 1300 | 39/28 | 40/29 | 41/30 | 43/31 | 44/32 | 45/33 | 46/35 | 48/36 | 49/37 |
| 1400 | 40/28 | 41/29 | 42/30 | 43/32 | 44/33 | 46/34 | 47/35 | 48/36 | 49/38 |
| 1500 | 40/29 | 42/30 | 43/31 | 44/32 | 45/33 | 46/35 | 48/36 | 49/37 | 50/38 |
a Numbers refer to average mean BP/10th percentile for mean blood pressure.
Another “normative range” often used to warrant intervention is a single absolute mean BP value chosen over a wide range of gestational ages. The most common is a mean BP less than 30 mm Hg. This approach is based on findings suggesting that the lower limit of the BP autoregulatory curve is around 28 to 30 mm Hg in neonatal animal models as well as preterm neonates. Munro and colleagues studied the relationship between mean arterial BP and cerebral blood flow assessed by near-infrared spectroscopy (NIRS) in 17 extremely preterm infants, 12 of whom were hypotensive and 5 were normotensive. Patients who were hypotensive had lower cerebral blood flow compared with normotensive infants. When dopamine was commenced in the hypotensive infants, the mean BP and cerebral blood flow increased. Cerebral blood flow correlated with mean arterial BP in hypotensive infants before ( R = 0.62) and during ( R = 0.67) dopamine administration, but not in normotensive infants. Using complex statistical analysis, the authors suggested a “breakpoint” of mean arterial BP of 29 mm Hg in the untreated cohort of infants. These findings need to be interpreted cautiously considering the small number of patients included and the lack of inclusion of potential confounders, including the effect of gestational age and the partial pressure of carbon dioxide. An interesting finding was that once dopamine therapy was commenced, cerebral blood flow seemed to continue along a pressure-passive curve, suggesting a loss of autoregulatory capacity even when BP increased beyond the lower autoregulatory elbow of 29 mm Hg. Greisen and colleagues explored the relationship between white matter injury and blood flow in 13 preterm infants using single-photon emission computed tomography with 99 Tc labeled hexa-methylpropylenamide oxime as the tracer. They found no statistically significant relationship between white matter blood flow percentage (WMBF%) and any of the variables studied, including mean arterial BP. However, using nonlinear regression assuming a plateau over a certain BP threshold and a positive slope below this threshold, the relation to WMBF% was statistically significant ( P = .02) with a threshold identified at 29 mm Hg (95% confidence interval 26 to 33 mm Hg). They concluded that periventricular white matter is selectively vulnerable to ischemia during episodes of low BP. There were a number of limitations to this study as well, including the small number of infants included; two imaging studies were performed in only 3 of the 13 infants, while the relation between BP and WMBF% was statistically significant, two-thirds of the variance of WM% was still unexplained. Interestingly, these values approximate to data published almost 30 years ago by Miall-Allen et al., showing that in 33 infants of less than 31 weeks’ gestation, a mean BP of less than 30 mm Hg for over an hour was significantly associated with severe intracranial hemorrhage, ischemic cerebral lesions, or death within 48 hours. No severe lesions developed in infants with a mean BP 30 mm Hg or greater. Accordingly, this value (30 mm Hg) is considered by some as a threshold to start intervention. However, these data need to be interpreted cautiously when applying this principle to those at greatest risk of brain injury, that is, the most immature preterm infants. Applying this principle to infants less than 26 weeks’ gestation would essentially mean intervening for a significant majority in the first postnatal hours. Indeed Greisen and colleagues state that their “result should not be used for clinical decision making.” Therefore, routine intervention based solely on maintaining a BP greater than 30 mm Hg for extreme preterm infants should be avoided.
Another “range” commonly used is that of the Joint Working Group of the British Association of Perinatal Medicine. They recommended that the mean arterial BP in mm Hg should be maintained at or greater than the mean gestational age in weeks. There is little published evidence to support this “rule,” but it remains the most common criteria used to define hypotension. Lee and colleagues identified that the lower limits of mean arterial BP for infants between 26 and 32 weeks’ gestation were numerically similar to the gestational age. The German Neonatal Network presented data recently on a very large cohort of preterm infants. They showed the lowest mean arterial BP recorded on day 1 was similar to the gestational age in weeks ( Table 3.2 ). However, there is growing evidence highlighting the inadequacy of this guideline. Cunningham et al. have shown a poor relationship between this rule and the incidence of intraventricular hemorrhage. Data collected by the Canadian Neonatal Network (CNN) show that over 52% of preterm infants less than 28 weeks’ gestation are “hypotensive” by this rule alone in the first postnatal day and, as such, may warrant intervention. This simple rule also needs to be interpreted cautiously in light of the normal increase in BP over the first days, especially during the first 3 days after delivery. What is clear is that this rule is very easy to remember and is consistently used by many to guide intervention.
| Gestational Age Weeks | Number of Infants With Data | Lowest Mean Arterial Blood Pressure (mm Hg; Median [IQR]) |
|---|---|---|
| 22 | 25 | 21 (18–25) |
| 23 | 178 | 21 (19–24) |
| 24 | 339 | 22 (20–25) |
| 25 | 431 | 24 (21–26) |
| 26 | 583 | 24 (21–28) |
| 27 | 666 | 26 (22–29) |
| 28 | 725 | 27 (24–31) |
| 29 | 725 | 29 (25–32) |
| 30 | 709 | 30 (27–34) |
| 31 | 526 | 31 (27–35) |
| All | 4907 | 27 (23–31) |
In summary, numerous reference ranges exist. Many of these are problematic, especially because of the lack of a consistent relationship between low BP values and clinically relevant short- and long-term outcomes, and because there are very few data on the effectiveness of the commonly used treatment modalities to decrease the incidence of peri/intraventricular hemorrhage (P/IVH) and white matter injury. However, consistent observations are that BP in the first postnatal days is gestation specific, typically characterized by a drop in the first hours after delivery followed by an increase thereafter over the first 3 days. The timing of intervention for low BP in preterm infants occurs on day 1 in over 90% of cases, regardless of gestational age. These factors need to be considered when evaluating BP values, whether one intervenes or not, and when designing future clinical trials in this area.
Clinical Factors Affecting Blood Pressure
Antenatal Steroids
Several investigators have reported that neonatal BP is higher in preterm infants whose mothers received antenatal steroids. Moise and colleagues studied the amount of BP support received by extremely preterm infants (23 to 27 weeks’ gestation) whose mothers did or did not receive antenatal steroids. Infants not exposed to antenatal steroids had lower mean BP values from 16 to 48 hours postnatally. Furthermore, the use of dopamine was increased in infants not exposed to antenatal steroids. Demarini and colleagues reported that mean BP values during the first 24 postnatal hours were higher in very low birth weight (VLBW) infants whose mothers received antenatal steroids, and that volume expansion and vasopressor support were decreased in those infants.
Elimian et al. evaluated whether incomplete courses of antenatal steroids were beneficial. After adjusting for gestational age, they found that one dose of betamethasone compared with none was associated with a significant reduction in the need for vasopressor-inotropes (odds ratio [OR], 0.35; 95% confidence interval [CI], 0.14, 0.85; P < .02) and the rate of P/IVH (OR, 0.42; 95% CI, 0.19, 0.92; P < .03). In a subsequent randomized trial comparing betamethasone versus dexamethasone, they found no difference in the incidence of need for vasopressor-inotrope use between the two corticosteroid preparations.
Placental Transfusion
A recent systematic review by Rabe et al. found a lower mean BP and a greater need for vasopressor-inotrope support in those who received immediate cord clamping compared with those who had delayed clamping. There were no measures of cardiac output presented in this review but Somers et al., in a nested cohort study of 51 preterm infants, found an increase in superior vena cava (SVC) flow measurement over the first 4 postnatal days. However, the results of the much larger Australian Placental Transfusion Study Echo Sub-Study found no difference in the incidence of low BP using the gestational age–based rule for 15 minutes, in the use of vasopressor-inotropes, and in flow measurements between the groups. A recent meta-analysis of umbilical cord milking (UCM) identified two studies that reported BP data. Systolic, diastolic, and mean BP were all significantly higher in the group who had UCM performed. However, there was significant heterogeneity in the studies. Katheria and colleagues found no significant difference in BP values between a group who received UCM versus immediate cord clamping, but did identify a significant difference in SVC flow over the first 24 postnatal hours. However, this did not translate into a difference in the need for volume, vasopressor-inotrope, or hydrocortisone therapy. A recent meta-analysis of UCM found that while UCM was associated with some benefits and no adverse effects in the immediate postnatal period in preterm infants, further studies were warranted to assess the effect of UCM on short- and long-term outcomes. Katheria and colleagues subsequently compared UCM with delayed cord clamping and found higher systemic blood flow with UCM compared with delayed cord clamping in preterm neonates delivered by cesarean section. The best summary of this evidence to date is that placental transfusion is associated with higher BP values, but the effects on flow are not as clearly evident and it is not certain which approach (delayed cord clamping or UCM) is superior in improving postnatal hemodynamic transition (see Chapter 4 , Chapter 5 ).
Respiratory Support
Kluckow and Evans observed a highly significant negative influence of mean airway pressure on mean BP in preterm neonates requiring mechanical ventilation. They subsequently highlighted the effects of an alteration of positive end expiratory pressure (PEEP) from 5 to 8 cm H 2 O in ventilated preterm infants and showed a significant reduction in right ventricular output with increased PEEP. Ventilation strategies that aim to avoid mechanical ventilation seem to have a lower incidence of low BP and low flow states. De Waal and colleagues described the hemodynamic variables in infants who had the INtubation, SURfactant, Extubation (INSURE) procedure and found an incidence of hypotension of 16% and rates of intervention at 10%. Similar data are presented for the Avoidance of Mechanical Ventilation Trial where 17% to 18% of patients had low BP overall. Although the evidence is primarily from cohort studies, it would appear that mechanical ventilation can have an adverse effect on cardiovascular status, likely by impeding venous return and thus cardiac filling, and should be a recognized potential cause of low BP and low systemic flow in preterm infants. There are two other potential effects associated with mechanical ventilation: tracheal suctioning and the use of sedation. Tracheal suctioning has been associated with alterations, predominantly increases, in mean BP. In addition, hypotension was associated with the use of morphine in the Neopain Trial. Therefore, strategies to minimize mechanical ventilation should form a critical part of the assessment and management of low BP in preterm infants.
Blood Pressure and Short- and Long-Term Outcomes
This remains one of the most contentious areas of BP management, as it is unclear at present whether low BP is indeed associated with adverse outcome, whether the interventions for low BP improve outcome, and whether the treatment itself is detrimental to the developing brain. It is difficult to answer any of these questions retrospectively, but these are the best data that we currently have available, considering the paucity of adequately powered clinical trials in this area. Numerous studies have highlighted an adverse relationship between low BP and short- and long-term outcome. We explored this relationship previously and highlighted some of the concerns in a systematic review of the literature at that time. There were 18 studies identified, including cohort and case-controlled studies with small numbers of patients—none of which were powered for long-term neurodevelopmental follow-up. There were a number of problems identified in this review—the majority of which will not be surprising to the reader. The definition of hypotension varied substantially across the studies, as did the outcome assessment used. The overall conclusion of the data from this review was that there is some association between having a lower BP and a worse outcome but that there were several potentially confounding factors that precluded one from drawing any strong inference from this association.
A number of important studies have been published since this review and raise further questions in relation to this association. Logan et al. evaluated three indicators of hypotension: (1) lowest MAP in the lowest quartile for gestational age; (2) treatment with a vasopressor-inotrope; and (3) BP lability. They found no association between any of these definitions and adverse outcome defined as white matter abnormality on cranial ultrasound at discharge. They found little evidence that these early postnatal hypotension indicators were associated with developmental delay at 24 months’ corrected gestational age. However, Batton and colleagues compared neurodevelopment in three cohorts of extremely preterm infants: those untreated with “normal” BP, untreated with “low” BP, and treated with low BP. Low BP was defined as MAP of less than 25 mm Hg on more than three occasions in the first 72 hours after delivery. Infants with low BP—regardless of treatment—had worse neurodevelopmental outcomes than infants with normal BP. They concluded that early low BP may be independently associated with a poorer outcome. Data from the CNN showed that infants with hypotension defined as a lowest BP less than their gestational age, or a BP less than the 10th percentile using the criteria of Watkins et al., were statistically more likely to develop severe P/IVH. However, this association was no longer apparent when vasopressor-inotropes were included in the model. A recent publication from the German Neonatal Network identified that hypotension during the first 24 postnatal hours was associated with adverse outcomes in VLBW infants. This study examined the lowest mean BP on the first postnatal day in over 4900 preterm infants less than 32 weeks’ gestation born in 47 centers throughout Germany. This retrospective study has many strengths, including a very large number of included infants and consistency in data entry and outcome definitions. On multivariate analysis, the minimum mean arterial BP during the first 24 postnatal hours was significantly associated with an increase in the odds of a P/IVH (OR, 0.97 mm Hg, CI, 0.95–0.99), suggesting again that low BP is associated with adverse outcome.
However, in a subsequent study, Batton et al. investigated the relationship between early BP changes, the receipt of antihypotensive therapy, and the outcomes for extreme preterm infants less than 27 weeks’ gestation at 18 to 22 months’ corrected age. Of 367 infants, 203 (55%) received an antihypotensive therapy, 272 (74%) survived to discharge, and 331 (90%) had a known outcome at 18 to 22 months’ corrected age. Early BP changes were defined by the expected rate of rise of 5 mm Hg over the first postnatal day. Accordingly, four groups of infants were identified: infants who did or did not receive antihypotensive therapy in whom BP did or did not rise at the expected rate. Interestingly, extremely preterm infants who received antihypotensive therapy in the first 24 hours after birth had a significantly higher rate of death or impaired neurodevelopment at 18 to 22 months’ corrected age compared with untreated infants irrespective of early changes in the BP. Van Bel found no association between a mean arterial BP less than gestational age in weeks and lower neurodevelopmental outcome scores at 24 months. However, they found that low regional cerebral oxygenation values were associated with lower neurodevelopmental outcome scores (see Chapter 18 ). This suggests that indirect assessment of end-organ blood flow and oxygen delivery (cerebral tissue oxygenation measure by NIRS) is important and might be more sensitive than mean BP values as a potential marker of long-term neurodisability (see Chapter 17 , Chapter 18 ). It is clear that the best approach would be to understand the status of both the systemic circulation (BP and cardiac output) and end-organ blood flow distribution (tissue oxygen delivery) to more appropriately evaluate the impact of transitional hemodynamics on short- and long-term outcomes (see Chapter 21 ).
While the issue of low BP and adverse outcome remains contentious, so too is the possibility that treatment (volume, vasopressor-inotropes, and/or inotropes) may be a contributing factor to adverse outcome. Earlier neonatal animal work has shown an association between intervention and adverse outcome. A number of recent publications exploring the relationship between hypotension and its treatment using retrospective data analysis have suggested that treatment itself may be detrimental. Fanaroff et al. found an association between “treated hypotension” and adverse outcome defined as delayed motor development, hearing loss, and death. Limperopoulos et al. found an association between volume expansion on the second day of life and abnormal cranial ultrasound findings. A study from the CNN published as an abstract also found no association between hypotension and adverse outcome when the use of vasoactive agents was included in the statistical model. Another interesting finding from this dataset was that patients who were normotensive as per the authors’ criteria, yet treated, had a worse outcome than infants who were hypotensive and not treated. There are two ways of interpreting this finding: treatment itself is detrimental or clinicians recognized other variables that warranted treatment, so a more global approach rather than reliance on BP targets directed the therapy received. Of course it is not possible to answer this question retrospectively. Batton et al. concluded that antihypotensive therapy exposure was associated with an increased risk of death/neurodevelopmental deficit at 18 to 22 months’ corrected age when other risk factors known to affect survival and neurodevelopment were controlled for. Although the German Neonatal Network study’s findings also found an association between treatment with vasopressor-inotropes in the first 24 hours of postnatal life and P/IVH (OR, 1.86, CI [1.43 to 2.42]; P < .001) in a multilogistic regression model, the authors emphasized that “vasoactive treatment might be due to complications, and is, therefore, not a completely independent cofactor.” In addition, this study, like others in this area, did not factor in the timing of the injury and the timing of the intervention.
As the potential negative effects of treatment itself remain a concern, they need to be prospectively studied. However, due to the lack of prospectively collected data and the findings of other studies showing different results, no definitive conclusion can be drawn at present. The follow-up study to a randomized prospective trial comparing the effectiveness of dopamine and epinephrine in increasing BP and cerebral blood flow in hypotensive VLBW neonates during the first postnatal day found that neonates responding to treatment had long-term neurodevelopment outcomes comparable to age-matched normotensive controls, and that non-responders had worse long-term neurodevelopmental outcomes. These findings suggest that treatment by careful, step-wise titration of vasopressor-inotropes may not be harmful. However, as the primary outcome measure of the original study was not long-term neurodevelopmental outcome, the follow-up study was not properly powered to address the concerns about vasoactive medication use and potential harm. A number of recent studies have also attempted to answer this question. Two ended early because of enrollment issues, namely the Hypotension in Preterms: Health Outcomes Protocol (HIPHOP) trial from Italy and the National Institute of Child Health and Human Development (NICHD) hypotension trial. The NICHD trial enrolled 10 patients from an eligible population of 120 patients. Factors contributed to the low overall rate of enrollment included the inability to obtain consent in a timely manner and physicians’ unwillingness to enroll. Informed consent for a trial of vasoactive medication use enrolling primarily in the first hours of postnatal life has many challenges. The Hypotension in Preterm Infants trial is currently enrolling, and the NEOCIRC trial is about to begin enrollment. Of note is that, in addition to the harm vasoactive medications might potentially directly exert, inappropriate titration of the medications itself might cause sudden increases and/or decreases in BP and cerebral blood flow in patients without effective cerebral blood flow autoregulation (see Chapter 2 ), as suggested by Greisen above, and thus might cause harm. The understanding of the challenges associated with titration of vasoactive medications is critical to the safe delivery of continuous infusions of these medications in this vulnerable patient population. This includes long lag times before the agent actually reaches the patient, resulting in both a delay in delivery and, potentially, unpredictable effects.
It is also interesting to note the wide variability in the incidence of hypotension and the incidence of intervention. Laughon and colleagues evaluated factors associated with intervention for hypotension in extremely low gestational age infants during the first postnatal week and found that neither the lowest MAP on the day of treatment nor other characteristics of the infants accounted for center differences in treatment. This suggested that the decision to intervene was more strongly associated with the center where the care was provided than with the particular infant attributes. This may reflect institutional practices. Subsequently, Batton and colleagues showed similar variation among centers but also highlighted significant variability in intervention rates based on low BP values alone. Antihypotensive therapy was often provided to infants without low BP and, paradoxically, not prescribed to infants with low BP. Antihypotensive therapy was administered to 28% to 41% of infants without BP values that most would consider low. In the study by Faust and colleagues, the overall rate of a low BP, using the less than gestational age definition, was 52%, yet the overall vasopressor-inotrope treatment rate on the first postnatal day was 9.3% (433/4675). The Australian Placental Transfusion Study’s Echo Sub-Study found an incidence of low BP also using the gestational age–based definition for at least a 15-minute duration, in greater than 30% of infants less than 30 weeks’ gestational age. However, the intervention rate was only around 11%. These three studies suggest that other factors are taken into consideration when clinicians decide on whether to intervene, based on low BP values. Hence the concept of permissive hypotension whereby one tolerates lower BP values if other parameters suggest that systemic and end-organ perfusion are appropriate. However, this approach carries the potential risk of delaying the initiation of treatment in patients whose perfusion may worsen to the point where it reaches the threshold of inadequate oxygen delivery. The most commonly used clinical criteria to evaluate end-organ perfusion are set out below, and other objective parameters are discussed in a later section.
Related posts:
 Assessment of Systemic Blood Flow and Myocardial Function in the Neonatal Period Using Ultrasound
Assessment of Systemic Blood Flow and Myocardial Function in the Neonatal Period Using Ultrasound
 Point of Care Ultrasound in the Assessment of the Neonatal Cardiovascular System
Point of Care Ultrasound in the Assessment of the Neonatal Cardiovascular System
 Tissue Doppler Imaging
Tissue Doppler Imaging
 Principles of Developmental Cardiovascular Physiology and Pathophysiology
Principles of Developmental Cardiovascular Physiology and Pathophysiology
 Speckle Tracking Echocardiography in Newborns
Speckle Tracking Echocardiography in Newborns
 Cardiac Magnetic Resonance Imaging in the Assessment of Systemic and Organ Blood Flow and the Function of the Developing Heart
Cardiac Magnetic Resonance Imaging in the Assessment of Systemic and Organ Blood Flow and the Function of the Developing Heart
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


