CHAPTER 7 Diagnostic Coronary Angiography
ANGIOGRAPHIC VIEWS
In most patients, the right coronary artery is best imaged with a combination of left lateral, cranial left anterior oblique (Cr-LAO), RAO, and Cr-RAO views. Although not used by many cardiologists, the lateral view (Fig. 7-1) has several advantages over a standard 60-degree LAO view because it usually allows better visualization of the mid right coronary artery and collaterals to the left anterior descending artery (LAD). The Cr-LAO view is necessary to lay out the posterior descending artery and posterolateral branches arising from the right coronary artery beyond the posterior descending artery (Fig. 7-2). In patients with large posterolateral branches, the Cr-RAO view projects the posterior descending artery and posterolateral branches clear of each other (Fig. 7-3). Usually, one should not use the Cr-RAO view to the exclusion of the RAO view (Fig. 7-4); however, because the body of the right coronary artery is foreshortened in the Cr-RAO view.
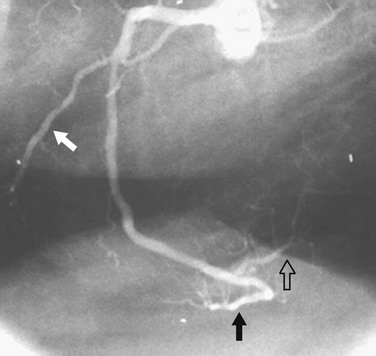
 FIGURE 7-1
FIGURE 7-1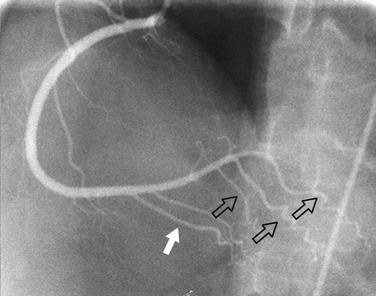
 FIGURE 7-2
FIGURE 7-2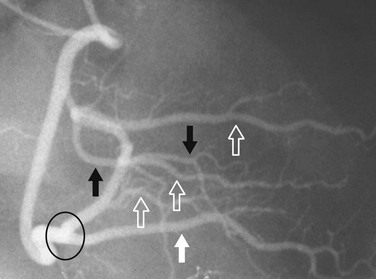
 FIGURE 7-3
FIGURE 7-3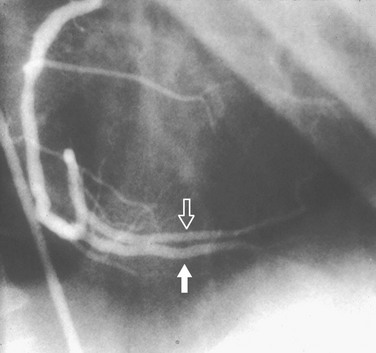
 FIGURE 7-4
FIGURE 7-4In the average patient, the left main coronary artery is projected at true length in either a posteroanterior or a shallow LAO view (Fig. 7-5). The bifurcation and proximal portions of the LAD and left circumflex artery are usually best seen in the Cr-LAO1 (Fig. 7-6) and RAO projections. Enough LAO rotation should be used to place the distal LAD between the spine and the diaphragm. In some individuals, the left main coronary artery has an up-going course. This requires using caudal angulation to eliminate foreshortening. The caudal LAO2 view is the only angiographic view that should be performed with the patient holding his or her breath in expiration (Fig. 7-7). If the patient inspires, the effect of the caudal angulation is negated; this is most common in large patients and requires more exposure than nonangulated views resulting in a degraded image. Because the distal LAD frequently is superimposed on the diaphragm in the Cr-LAO view, a lateral view is often useful (Fig. 7-8).
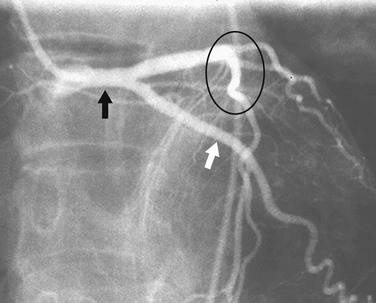
 FIGURE 7-5
FIGURE 7-5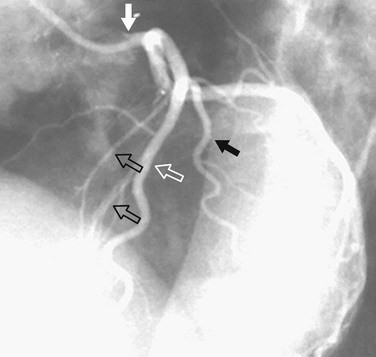
 FIGURE 7-6
FIGURE 7-6


