Fig. 11.1
Beach chair position for shoulder arthroscopy
For the lateral decubitus position, the patient is positioned laterally on a padded table with the operative side up. Commonly, a bean bag support is used to aid with positioning and keep the patient stable in the desired position; alternatively, padded anterior and posterior positioner pads that attach directly to the table can be employed to stabilize the patient’s torso. Adequate padding is important to prevent skin and neurologic complications. In addition, an axillary roll is placed under the nonoperative arm to limit pressure over the brachial plexus and vascular supply to the limb. The head should be secured in a neutral position and the contralateral elbow and knees in flexion. The surgical arm is then placed in a sling with longitudinal traction. Commonly, a pulley system is used where the surgical arm is suspended in the air by a sling connected by a rope, through a pulley, to a stack of traction weights. The amount of traction weights used is roughly based on the size of the patient (Fig. 11.2). Hennrikus et al. discussed the importance of the ischemic consequences of shoulder traction as it can cause neuropraxia and markedly reduce local and distal tissue perfusion [12]. Regardless of arm position, Peruto et al. suggest traction should be limited to 15–20 lb. [13]. An additional sling attached to the upper arm can be used to assist with lateral traction to the operative extremity. In order to improve orientation and visualization, Gross and Fitzgibbons modified the lateral decubitus position by tilting the table 20–30° posteriorly [14]. This modified position made the glenoid parallel to the floor, thereby improving visualization and making the relationship of structures more constant. Klein et al. studied the effect of arm position on brachial plexus strain and found that 45° of flexion combined with either 0 or 90° of abduction maximized visibility while minimizing strain [15].

Fig. 11.2
Lateral decubitus position for should arthroscopy
Advantages and disadvantages of the beach chair position and the lateral decubitus position are highlighted in Table 11.1.
Table 11.1
Beach chair vs. lateral decubitus
Beach chair | Lateral decubitus | |
|---|---|---|
Advantages | – Upright, anatomic position – Decreased incidence of nerve injury – Decreased risk of neurovascular complications during portal placement – Easier conversion to an open procedure utilizing deltopectoral approach – Easier exam under anesthesia – Can mobilize operative arm easier | – Increased visualization of the glenohumeral joint and subacromial space due to joint distraction – No additional traction assistance needed – Lateral distraction of the GH joint allows easier access to the posterior and inferior GH joint |
Disadvantages | – Maintenance of cerebral perfusion – Intraoperative hypotension – Airway complications – More difficult to access posterior shoulder pathology – Cost (if using arm holder) | – 10 % incidence of nerve injury with traction – Nonanatomic orientation – Poorer tolerance of regional anesthesia |
Pertinent Shoulder Anatomy and Portal Locations
Following prepping, draping, and setup in either the lateral decubitus or beach chair position, the bony landmarks are palpated and marked. First, mark the posterolateral edge of the acromion. Then, the following landmarks should be marked: scapular spine, acromion, clavicle, coracoid, and AC joint. Accurately identifying and marking these landmarks is important as anatomical correlations and nerve/vascular anatomy is defined with respect to these landmarks. Knowledge of the locations and courses of nerve and vascular structures is important for portal placement and minimizing injuries.
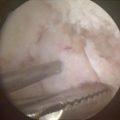
There are three primary portals and many secondary portals that can be used in shoulder arthroscopy cases (Fig. 11.3). These various portals are used for better visualization of certain structures and pathology or for assistance in certain procedures. See Table 11.2 for portal use by common procedures.

Fig. 11.3
Intraoperative photograph of a prepped and draped shoulder with anatomical landmarks and select portal locations. A, clavicle; B, coracoid; C, acromion; D, scapular spine; 1, posterior portal; 2, anterior portal; 3, low anterior portal for Bankart repair; 4, anterosuperior portal; 5, low anterolateral tenodesis portal; 6, lateral portal; 7, posterolateral portal; 8, Neviaser (supraspinatus) portal
Table 11.2
Portal use by common procedure
Procedure | Posterior | Anterior | Lateral | Posterolateral | Anterosuperior | Anteroinferior (5 o’clock) | Posteroinferior (7 o’clock) | Anterolateral (Port of Wilmington) | Neviaser | Axillary pouch | Inferolateral (pec-portal) |
|---|---|---|---|---|---|---|---|---|---|---|---|
Diagnostic arthroscopy | + | + | − | − | − | − | − | − | − | − | − |
Rotator cuff repair | + | + | + | + | − | − | − | − | − | − | − |
Subacromial decompression | + | + | + | – | – | – | − | − | − | − | − |
Anterior labral repair | + | − | − | − | +/– | + | – | – | – | − | − |
Multidirectional instability | + | − | − | +/− | + | + | − | − | + | − | |
SLAP repair | + | + | – | – | + | – | − | +/1 | − | − | − |
Biceps tenodesis | + | + | – | – | – | – | − | − | − | − | + |
Distal clavicle excision | + | + | + | + | – | – | − | − | − | − | − |
Primary Portals
1.
Posterior: The posterior portal is the primary viewing portal and the first portal established in diagnostic shoulder arthroscopy. It is located 2 cm inferior and 1–2 cm medial to the posterolateral corner of the acromion. A skin incision is made, followed by a blunted arthroscopic obturator and its sheath directed toward the coracoid tip. This can either pass through the substance of the infraspinatus muscle or pass between the infraspinatus and teres minor. It is usually located in the “soft spot” between the humeral head and the glenoid posteriorly. Proper portal placement is important to decrease injury risk to the axillary and suprascapular nerves. According to a study by Meyer et al., the posterior portal is located an average 49 mm from the axillary nerve and 29 mm from the suprascapular nerve [16].
2.
Anterior: The anterior portal is an essential working portal in most shoulder arthroscopy procedures. It is located just lateral to the coracoid process and anterior to the AC joint. The portal passes between the pectoralis major and deltoid muscles. The portal is usually placed under direct supervision from the posterior portal with the aid of a spinal needle. The needle is placed within the rotator interval using an outside-in technique. Care must be taken to ensure that all anterior portals are lateral to the coracoid in order to minimize the risk of neurovascular injury to the brachial plexus and axillary vessels. A study by Lo et al. found that, on average, the musculocutaneous nerve lies approximately 33 mm inferior to the tip of the coracoid [17].
3.
Lateral: The lateral portal, primarily used for procedures in the subacromial space and to address AC pathology, is located 2–3 cm lateral to the lateral edge of the acromion. The portal passes through the deltoid muscle. As with all portals, the location may be adjusted based on pathology. A study by Burkhead et al. found that the axillary nerve can be found as close as 31 mm distal to the anterolateral border of the acromion so care should be taken not to make this portal too inferior [18].
Secondary Portals
4.




Posterolateral: The posterolateral portal is primarily utilized for subacromial decompression, rotator cuff, and labral repairs. It is located 2–3 cm lateral to the posterolateral edge of the acromion. Using an outside-in technique, the portal is made and the trocar is aimed medial to the subacromial bursa [16]. Inferior placement places the axillary nerve at risk.
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
