Diaphysis
Johnny U. V. Monu
Thomas L. Pope Jr.
GENERAL CONSIDERATIONS
Diaphyseal lesions are unique because of their location, their frequent indirect but significant bearing on related joints, and their intimate association with peripheral arteries and nerves. Lesions involving the diaphyseal region of all the long bones are considered in this chapter.
RADIOGRAPHIC EXAMINATION
The routine radiographic examination of the long bones must include both frontal and lateral projections. A single projection of a long bone is an inadequate radiographic study (Fig. 23.1) except in the severely injured patient, and then only neurologic or hemodynamic instability or possible acute traumatic aortic injury should take precedence. Prior to definitive evaluation, however, radiographs of the long bones in orthogonal planes must be obtained to provide the necessary data on which management decisions can be made.
It is equally fundamental to include the entire long bone(s) in the examination whenever possible. When not possible, for whatever reason, the joint closest to the site of injury must be included in the examination. The purpose of the “closest joint” tenet is to be able to accurately localize the injury and to identify concomitant injuries that frequently occur close to or involve the joint (Fig. 23.2).
Shortening of one of the bones of the forearm or leg as a result of angulation or overlap of fragments can be accommodated only by either a fracture or dislocation of the other bone. Therefore, when one of the bones of the forearm or leg is shortened as a result of fracture, it is imperative to examine the entire part radiographically to diagnose the fracture or dislocation that must involve the other bone (Figs. 23.3 and 23.4).
The distal fragment of midfemoral or midtibiofibular fractures may be externally rotated as much as 90 degrees. This feature may not be appreciated unless the entire part is included in the radiographic study (Fig. 23.5).
Thus, radiographic reports of diaphyseal fractures should address the fracture pattern, the bone quality, and the presence of bone loss especially if there is comminution, the amount of limb shortening, and the presence of air in the soft tissues.
The most commonly accepted convention for describing the relationship of the fragments of long or short tubular bones is to relate the position of the distal fragment to that of the proximal fragment. Alignment is the relationship of the longitudinal axis of the distal fragment to that of the proximal fragment. If the long axis of each fragment is parallel, alignment is said to be normal. Displacement refers to translation of the distal fragment in any direction with respect to the proximal fragment without angulation. “Angulation” indicates that the long axis of the distal fragment is canted (angled) with respect to the long axis of the proximal fragment. A distal fragment may be displaced, angled, or displaced and angled (Fig. 23.6) with respect to the proximal fragment. Proximal retraction of the distal fragment
with respect to the proximal is referred to as overriding (Fig. 23.6).
with respect to the proximal is referred to as overriding (Fig. 23.6).
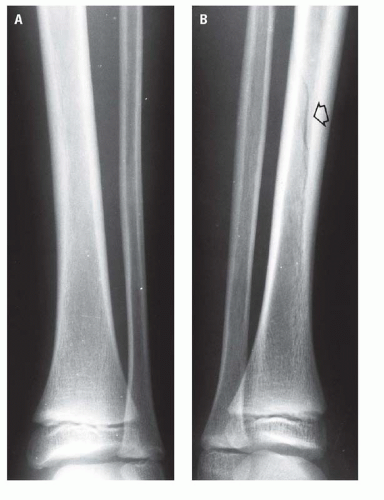 Figure 23.1. A: The frontal radiograph of the leg could very easily be interpreted as “negative.” B: The lateral projection clearly demonstrates the minimally displaced oblique fracture in the middle third of the tibia (arrow). |
 Figure 23.2. Transverse fracture in the midshaft of the humerus with an associated proximal humeral physeal injury. |
A segmental fracture is one in which two fractures occur at disparate locations within the same long bone, resulting in a separate and discrete fragment that is not attached to either the proximal or the distal fragment. The separate fragment is the “segment” of a segmental fracture (Fig. 23.7).
Peripheral Doppler ultrasound and computed tomography angiography (CTA) play an important role in the evaluation of traumatic lesions of the extremities. Although it is the responsibility of the attending physician to specifically evaluate the circulation of an injured extremity, it is equally the responsibility of the radiologist to identify and indicate to the attending physician those injuries that, because of the normal anatomic relationship between the arteries and the bones, have the potential for associated vascular involvement. However, the “proximity of wound” alone is not an indication for emergent CTA in the presence of an otherwise clinically normal extremity. Obviously, clinical signs or symptoms of arterial compromise distal to either a penetrating injury or a displaced long bone fracture
require at least consideration of CTA or peripheral angiography. The priority of the CTA or angiogram and where it is performed (e.g., the emergency center, the angiography suite, the operating room) must be determined jointly by the attending physician and the radiologist based on the patient’s overall condition and the availability of angiographic facilities.
require at least consideration of CTA or peripheral angiography. The priority of the CTA or angiogram and where it is performed (e.g., the emergency center, the angiography suite, the operating room) must be determined jointly by the attending physician and the radiologist based on the patient’s overall condition and the availability of angiographic facilities.
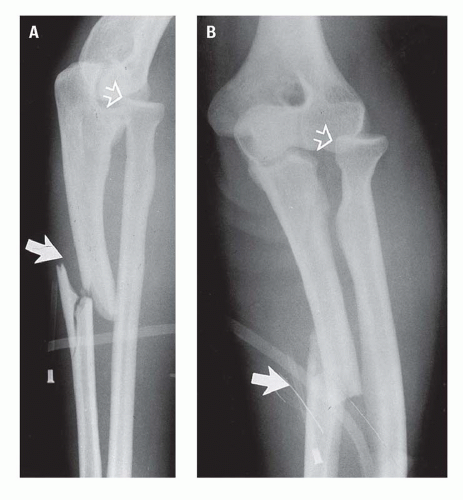 Figure 23.3. Bado type III Monteggia fracture. Shortening of the ulna due to overriding (A) and angulation (A,B) of its proximal fracture (solid arrow) has contributed to the anterolateral dislocation of the radial head (open arrow). |
 Figure 23.4. A: Complete fracture of the midshaft of the radius with shortening resulting from overriding of its fragments (straight arrow). The complete ulnar fracture (curved arrow) is impacted. B: The radial shortening has resulted in distal radioulnar diastasis (open arrow). |
 Figure 23.5. Approximately 90-degree external rotation of the distal femoral fragment. A: On the frontal radiograph, the hip is in the anteroposterior position, whereas the distal femoral fragment is in nearly true lateral position. B: On the horizontal beam lateral radiograph obtained with the patient supine, the proximal fragment is in lateral position, whereas the distal fragment is seen in frontal view. |
RADIOGRAPHIC ANATOMY
The contour of the part and the configuration of the soft tissues are important aspects of the radiographic evaluation of the extremities. Normally, adipose or loose areolar tissue is present adjacent to or surrounding the soft tissue structures of the extremities. In properly exposed radiographs, the muscles and fascial planes may be visible as linear or curvilinear radiolucent shadows.
RADIOGRAPHIC MANIFESTATIONS OF TRAUMA
Humerus
Fractures of the shaft of the humerus occur less frequently than fractures of the proximal end of the bone and are usually the result of direct trauma. Frequently, the humerus may be fractured by indirect force, such as a fall on the hand or elbow. Fractures of the proximal portion of the humerus caused by muscular action alone occur rarely.
Humeral shaft fractures are usually either oblique (Fig. 23.8) or transverse (Fig. 23.2). Displacement of the fragments is common, with the direction and magnitude of displacement due to (1) the direction and magnitude of force causing the injury and (2) the action of the muscles that insert on the humerus and their relation to the fracture site. Generally, if
the fracture line is located distal to the insertion of the deltoid muscle, the proximal fragment tends to be retracted outward, whereas the muscles of the arm draw the distal fragment upward. When the fracture is above the insertion of the deltoid, the distal fragment will be drawn laterally, and the proximal fragment medially by the unopposed action of the pectoralis, the latissimus dorsi, and the teres major muscles.
the fracture line is located distal to the insertion of the deltoid muscle, the proximal fragment tends to be retracted outward, whereas the muscles of the arm draw the distal fragment upward. When the fracture is above the insertion of the deltoid, the distal fragment will be drawn laterally, and the proximal fragment medially by the unopposed action of the pectoralis, the latissimus dorsi, and the teres major muscles.
 Figure 23.6. Displaced, angled fracture at the junction of the proximal and middle thirds of the femoral shaft. The distal femoral fragment is both medially displaced and angled with respect to the proximal fragment. |
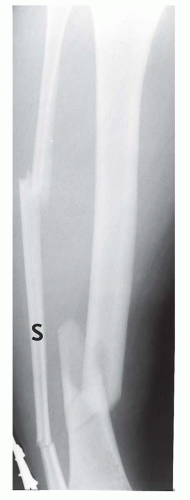 Figure 23.7. Segmental fracture. The separate fragment (S) between the proximal and distal fibular fractures constitutes the segmental fragment. |
The radial nerve lies in the musculospiral groove of the humerus. Consequently, radial nerve paralysis is the principal complication of humeral shaft fractures. Occasionally, other entrapment neuropathies may result following fractures. These fractures are typically found in the proximal to middle third of the humeral shaft (Fig. 23.9). Open fractures occur in less than 10% of humeral shaft fracture. Such injuries are often due to high-velocity trauma, and frequently, the fracture may be comminuted and radial nerve palsy and other systemic injuries may be present.
Radius and Ulna
The pronator quadratus sign, described in conjunction with injuries of the wrist, is extremely valuable in the detection of minimally displaced fractures of the distal diaphysis of the ulna (Fig. 23.10) or of the radius.
Isolated ulnar fractures or “nightstick” fractures (Fig. 23.11) are usually the result of direct trauma. The alignment of the fragments reflects the direction of the causative force.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


