Diffuse Lung Disease Associated with Lipid: Exogenous Lipid Pneumonia and Alveolar Proteinosis
W. Richard Webb
ENDOGENOUS LIPOID PNEUMONIA
Lipoid pneumonia (lung consolidation containing lipids) may be endogenous or exogenous. Endogenous lipoid pneumonia may occur due to bronchial obstruction with accumulation of lipid-rich cellular debris distal to the obstructing lesion; this is sometimes termed “golden pneumonia” because of its yellow color at gross pathology. The term “postobstructive pneumonia” usually suffices for this condition.
EXOGENOUS LIPOID PNEUMONIA
Exogenous lipoid pneumonia results from the chronic aspiration or inhalation of animal, vegetable, or petroleum-based oils or fats (Table 20-1). Petroleum-based oil (mineral oil) aspiration is most common, usually associated with its use as a laxative. Responsible animal-based oils (e.g., cod-liver and shark-liver oils, clarified butter) and vegetable-based oils are usually aspirated during ingestion or because of esophageal motility abnormalities with reflux.
TABLE 20.1 Exogenous Lipoid Pneumonia | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Acute aspiration results in an aspiration pneumonia. Chronic aspiration results in lipoid pneumonia associated with variable fibrosis and inflammation. The degree of lung inflammation or fibrosis associated with the aspirated oil is related to the amount of free fatty acid present. Animal fats generally result in more inflammation and fibrosis than vegetable or mineral oils because they are hydrolyzed by lung lipases, releasing fatty acids.
A large quantity of oily material must usually be aspirated over a period of time before symptoms develop. Symptoms include cough, mild fever, and chest discomfort; they are least common with mineral oil aspiration. Fat may be identified in the sputum in some patients.
Radiographic and CT Findings
Consolidation, ill-defined masses, or sometimes findings of fibrosis are seen on chest radiographs (Figs. 20-1A, 20-2A, and 20-3A). A lower-lobe distribution is typical but not always present. Opacities may be bilateral or unilateral. The radiographic appearance is nonspecific.
CT shows masses that may be well-defined or ill-defined, or areas of consolidation. As on chest radiographs, these areas tend to have a lower-lobe predominance and are often bilateral. A dependent location is also typical. Bronchi may be seen leading to the abnormal areas.
If a large amount of lipid has been aspirated, CT can show areas of low-attenuation consolidation (-35 to -75 HU) or low-attenuation regions within larger masses (see Figs. 20-1B to E and 20-2B); this appearance is most common in patients with chronic mineral oil aspiration. Because inflammation or fibrosis accompanies the presence of the lipid material, the CT attenuation of the consolidation or mass need not be low, but often small areas of low-attenuation oil are visible (see Figs. 20-1D and E, and 20-2B). In some patients, necrosis and cavitation are present.
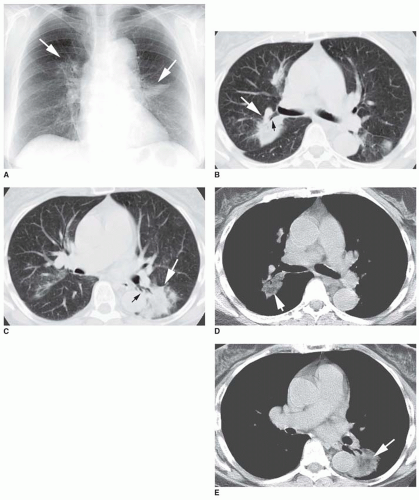 FIG. 20.1. Exogenous lipoid pneumonia resulting from chronic mineral oil aspiration. A: Chest radiograph shows irregular masses (arrows) in both lungs. B: CT shows an irregular mass (white arrow) in the posterior right upper lobe. This mass is dependent in location, and the posterior segmental bronchus of the right upper lobe (black arrow) leads to it. Several other nodular opacities are also seen. C: An ill-defined area of consolidation is visible in the superior segment of the left lower lobe (white arrow). It is dependent, and branches of the superior segment bronchus (black arrow) lead to it. D and E: Soft-tissue window scans at the same levels as (B) and (C) show low attenuation (-75 HU; arrows) within these masses. |
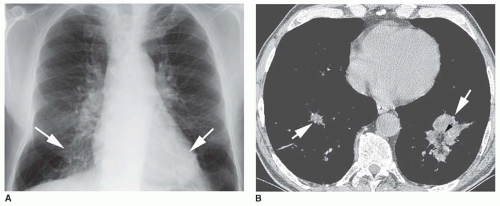 FIG. 20.2. Exogenous lipoid pneumonia resulting from chronic mineral oil aspiration. A: Chest radiograph shows irregular consolidation (arrows) in both lower lobes. B: CT shows irregular masses (large arrows) in both lower lobes. The left lower-lobe mass shows low attenuation (-100 HU; small black arrow) within the mass, although most of the mass appears to be of soft-tissue attenuation.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|