Diffusion tensor (DT) MR imaging is able to detect and quantify multiple sclerosis (MS)–related tissue damage within and outside T2-visible lesions. DT MR imaging has also been shown to be sensitive to the evolution of MS damage over time and to provide in vivo correlates of MS clinical severity and paraclinical markers of long-term disease evolution. Recent developments of DT MR imaging postprocessing techniques, such as tractography and voxelwise analysis, are likely to improve our understanding of the mechanisms associated with the accumulation of disability in MS. Important issues remain to be addressed, such as a detailed definition of the actual features underlying diffusion changes in MS and the potential of the technique in the differential diagnosis of MS.
Diffusion MR imaging has been largely used to study multiple sclerosis (MS), because of its ability to detect and quantify disease-related pathology of the central nervous system (CNS). The characteristics of diffusion, which can be defined as the random translational motion of molecules in a fluid system, are influenced by several CNS tissue components, including cell membranes and organelles. The MR imaging–measured diffusion coefficient of healthy CNS tissues is, therefore, lower than that in free water; it is called the apparent diffusion coefficient (ADC). Pathologic processes that result in a decrease of restricting barriers can determine an increase of the ADC values. Because the magnitude of diffusion also depends on the direction in which it is measured, its full characterization can be obtained in terms of a diffusion tensor (DT), a matrix that accounts for the correlation existing between molecular displacement along orthogonal directions. From the DT, it is possible to derive some parameters, which are quantitative and invariant to the frame choice: the mean diffusivity (MD), which measures the average molecular motion independent of any tissue directionality, and some other dimensionless indices of anisotropic diffusion, including fractional anisotropy (FA), which reflect the prevalence of diffusivity along one spatial direction (eg, along axonal fibers rather than perpendicular to them). The main postmortem correlates of diffusivity changes in MS are demyelination and axonal loss. Correlation with pathologic features is stronger for anisotropy than for diffusivity indices in the brain and spinal cord of patients who have MS.
This article discusses the main clinical applications of DT MR imaging to the study of MS and the role of new acquisition schemes and postprocessing methods.
Diffusion tensor MR imaging features of multiple sclerosis–related tissue damage
In MS, the first diffusion MR imaging studies consistently reported increased ADC values within both T2-visible lesions and the normal-appearing white matter (NAWM). These studies were affected by several limitations, however, including limited brain coverage, low number of encoded directions, and high susceptibility to motion artifacts. During the subsequent years, thanks to the development of more sophisticated acquisition schemes and the application of novel postprocessing techniques, DT MR imaging has been increasingly applied to the study of MS-related tissue damage with encouraging results.
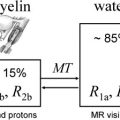
DT MR imaging has proved to be a valuable tool for investigating the variety of pathologic features of T2-visible lesions. In focal lesions, diffusion abnormalities (ie, increased MD and decreased FA) are always more pronounced than in the NAWM; however, their values are highly heterogeneous (see Ref for a review). The more severe abnormalities have been found in T1 hypointense lesions (also known as “black holes”), which represent areas of irreversible tissue disruption, gliosis, and axonal loss. Conversely, when comparing enhancing versus nonenhancing lesions, conflicting results have been reported; hence, how much DT MR imaging–detectable tissue disorganization within acute lesions is permanent (ie, related to neurodegeneration) and how much is transient (ie, related to edema, demyelination, and remyelination) remains an unsolved issue. A longitudinal study of enhancing MS lesions, which were followed up for 1 to 3 months, has shown that MD values were increased in all lesions, but continued to increase during follow-up only in a subgroup of them. This finding highlights that contrast enhancement does not allow us to profile acute MS lesions that are characterized by varying degrees of tissue disruption. In the same study, increased MD values were correlated with a greater degree of T1 hypointensity. Interestingly, a recent DT MR imaging study showed that cortical lesions have higher FA values than the normal-appearing gray matter (GM). This paradoxical finding may actually reflect the intralesional loss of dendrites and activation of microglial cells, thereby highlighting the potential contribution of DT MR imaging to help disentangle the pathologic features of GM lesions. More recently, the relationship between T2 relaxation times and DT MR imaging measures was investigated in a sample of MS lesions: lesions with long T2 fraction demonstrated the most pronounced diffusivity abnormalities, which were highly correlated with decreased myelin water content. When considered together, these findings support the notion that DT MR imaging may represent a technique able to assess the severity of functionally relevant tissue damage within MS lesions.
Outside T2 lesions, DT MR imaging discloses the presence of abnormalities in the NAWM and GM of patients who have MS, even before the development of new plaques. DT MR imaging is likely to be sensitive to the more disabling features of MS pathology in the NAWM, because diffusion abnormalities are more pronounced with increasing disease duration and neurologic impairment. NAWM and GM damage is only partially correlated with the extent of focal lesions and the severity of intrinsic lesion damage, suggesting that diffusivity changes in normal-appearing tissues are not entirely dependent on retrograde degeneration of axons transected in T2-visible lesions. The results of a recent study correlating diffusivity measures with perfusion findings in the corpus callosum of patients who had relapsing-remitting (RR) MS are more consistent with what would be seen in primary ischemia than in secondary hypoperfusion attributable to Wallerian degeneration.
DT MR imaging is also useful to assess the evolution of MS damage over time. Changes of DT MR imaging metrics seem to be independent of the concomitant accumulation of T2 lesions and reduction of brain tissue volume. Moreover, DT MR imaging might be more sensitive to detect the accrual of GM damage than that of NAWM, because it is the earliest clinical stage of MS. The application of DT MR imaging in monitoring the evolution of MS-related tissue damage over time therefore holds promise for trials aiming at assessing the efficacy of neuroprotective therapies.
Clinical correlations
DT MR imaging features and clinical severity of patients who have established MS are shown to be interrelated, the strongest associations being those related to the diffusion characteristics of T2 lesions and GM. The absence or mildness of DT MR imaging abnormalities in the normal-appearing brain may accompany a favorable clinical status, as suggested in patients who have pediatric MS. Because the accumulation of damage in focal lesions and NAWM occurs even during the earliest nondisabling phases of MS and this does not seem to be the case, at least at the same extent, for GM, GM diffusivity changes may be viewed as a hallmark of the more disabling and progressive stages of the disease. GM diffusivity features have also been related to the neuropsychologic profile of patients who have MS. In patients who had the benign form of MS, the severity of GM damage associated with cognitive impairment was similar to that observed in patients who had progressive MS and irreversible locomotor disability. Two other studies correlated DT MR imaging findings with the presence and severity of fatigue in patients who had MS. Disappointingly, the average MD and FA from brain, GM, and T2 lesions were not different between fatigued and nonfatigued patients, nor there was a correlation between any of these quantities and the fatigue severity scale scores. Apart from being used as stand-alone paraclinical measures, DT MR imaging can contribute to composite MR-based scores able to explain a large part of the variance of MS-related disability. Moreover, the results of a follow-up study of patients who had primary progressive (PP) MS suggest that the severity of diffusion abnormalities in GM may predict disability worsening 5 years later. Further larger, prospective studies are now warranted to ascertain whether DT MR imaging–derived measures of tissue damage might be used as paraclinical markers of MS prognosis.
Clinical correlations
DT MR imaging features and clinical severity of patients who have established MS are shown to be interrelated, the strongest associations being those related to the diffusion characteristics of T2 lesions and GM. The absence or mildness of DT MR imaging abnormalities in the normal-appearing brain may accompany a favorable clinical status, as suggested in patients who have pediatric MS. Because the accumulation of damage in focal lesions and NAWM occurs even during the earliest nondisabling phases of MS and this does not seem to be the case, at least at the same extent, for GM, GM diffusivity changes may be viewed as a hallmark of the more disabling and progressive stages of the disease. GM diffusivity features have also been related to the neuropsychologic profile of patients who have MS. In patients who had the benign form of MS, the severity of GM damage associated with cognitive impairment was similar to that observed in patients who had progressive MS and irreversible locomotor disability. Two other studies correlated DT MR imaging findings with the presence and severity of fatigue in patients who had MS. Disappointingly, the average MD and FA from brain, GM, and T2 lesions were not different between fatigued and nonfatigued patients, nor there was a correlation between any of these quantities and the fatigue severity scale scores. Apart from being used as stand-alone paraclinical measures, DT MR imaging can contribute to composite MR-based scores able to explain a large part of the variance of MS-related disability. Moreover, the results of a follow-up study of patients who had primary progressive (PP) MS suggest that the severity of diffusion abnormalities in GM may predict disability worsening 5 years later. Further larger, prospective studies are now warranted to ascertain whether DT MR imaging–derived measures of tissue damage might be used as paraclinical markers of MS prognosis.
Novel strategies
Diffusion Tensor MR Imaging of the Optic Nerves and Spinal Cord
Diffusion imaging of the optic nerve and spinal cord are technically more challenging than that of the brain, and studies of these structures are therefore still limited. The development of novel DT MR imaging sequences has recently made it possible to achieve an accurate estimate of the extent of damage in these regions, however. In the optic nerve, DT MR imaging measures provide an indication of the structural integrity of axons, and are correlated with neurophysiologic findings and, at a lesser magnitude, with clinical measures of visual functioning. DT MR imaging of the cervical cord provides measures of the global diffusivity and anisotropy status in this structure, which is known to play a major role for the locomotor abilities of patients who have MS. A DT MR imaging study of the cervical cord of patients who had RRMS and secondary progressive (SP) MS has shown that patients who have MS have MD and FA histogram characteristics suggestive of diffuse cord damage. In the same study, a multivariate linear regression model retained cord average FA and brain average MD as variables independently influencing patients’ clinical disability. Patients who have PPMS also have abnormal diffusivity and anisotropy of the cervical cord. When compared with SPMS, patients who had benign MS showed a milder cervical cord damage. Moreover, in patients who had benign MS, both cord cross-sectional area and FA were factors independently associated with the degree of clinical disability, thus suggesting that DT MR imaging may contribute to a comprehensive assessment of spinal cord damage. Likewise, DT MR imaging of the cervical cord may contribute to better characterized spinal cord damage of Devic neuromyelitis optica. Recently, a 2-year follow-up conventional and DT MR imaging study involving a large cohort of patients who had MS showed that both progressive atrophy and damage to the remaining tissue occur in the cervical cord. These two components of cord damage were not strictly interrelated. MS cord pathology was also found to be independent of concomitant brain changes, to develop at different rates according to disease phenotype, and to be associated with medium-term disability accrual. Cervical cord DT MR imaging in combination with proton MR spectroscopy has also been found to provide a reliable account of the cord damage occurring in patients who have spinal relapses.
Tractography
DT MR imaging tractography exploits the fact that axonal structures constitute a barrier to water diffusion, making it much more free along the axis of the fibers than perpendicular to it. By tracking the principal diffusion direction (ie, the direction of the primary eigenvector of the DT), nervous pathways can be reconstructed. DT MR imaging tractography, therefore, is a promising technique for in vivo segmentation of the major WM tracts in the brain ( Fig. 1 ). Some limitations prevent tractography algorithms from reconstructing the correct trajectories when more complex architectures than a single orientationally coherent fiber bundle are assessed. One of these limitations is intrinsic to the use of the tensor to model the diffusion process, which causes the principal diffusion direction not to follow the “real” fiber axes when fibers cross, but rather a direction that is the result of averaging between these crossing fibers. The poor spatial resolution of echo planar imaging, at present the most widely used technique for DT MR imaging, and the low signal-to-noise ratio of the acquired data also contribute to making the correct reconstruction of fiber bundles a challenging task. Furthermore, the application of tractography to the study of patients who have MS suffers from the drawback that the disease causes both focal and diffuse alterations of tissue organization, which result in a decreased anisotropy and a consequent increase in uncertainty of the primary eigenvector of the DT. A possible approach to overcome this problem is the use of probability maps of tracts of interest obtained from healthy subjects to assess DT MR imaging metrics from the corresponding patients’ tracts.