Chest wall infections originate in place or are transmitted from the intrathoracic space. Bacterial inflammation is usually accompanied by pain and clinically manifest inflammatory symptoms. Imaging is only needed if there is clinical suspicion of involvement of the bones or intrathoracic compartments. CT is valuable for diagnostic exploration of any intrathoracic transmission of infection, while MRI lends itself to investigation of osteomyelitis.
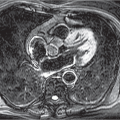
If severe local findings are in contrast to a mild clinical presentation, the possibility of a tuberculous abscess should be considered. This results from per continuitatem spread of tuberculous pleuritis and is known as “empyema necessitans” (or “empyema necessitates”). The resultant tuberculous chest wall abscesses may be very large (▶Fig. 13.1).
13.2 SAPHO Syndrome
At times, palmoplantar pustulosis of the skin as well as severe acne are seen in association with characteristic skeletal findings, in particular in the chest wall. The acronym “SAPHO syndrome” was coined to denote this combination of synovitis, acne, palmoplantar pustulosis hyperostosis, and osteitis.
The clinical presentation reflects the combination of psoriasis, spondyloarthritis, and sterile multifocal osteomyelitis. The etiology is unknown. The vast majority of the osseous changes are observed in the anterior upper chest wall, especially in the sternocostoclavicular region. There may additionally be arthritis of the adjacent joints. Other findings such as osteosclerosis of one or several vertebral bodies or sacroiliitis may be present.1
Imaging demonstrates sclerosis and bulging of the medial ends of the clavicle and first rib as well as similar changes in the manubrium sterni (sternocostoclavicular hyperostosis, ▶Fig. 13.2). Often, erosions or ankylosis of the sternoclavicular joints are identified in addition to abnormal ossification on CT.2
Fig. 13.1 Tuberculous chest wall abscess.CT image. Transmission of inflammation from the pleural space (arrows) in a case of tuberculous pleuritis, known as “empyema necessitans.”
Fig. 13.2 SAPHO syndrome. Typical sternocostoclavicular hyperostosis. (a) Radiograph, sectional magnification. Increased sclerosis and bulging of the left medial end of the clavicle and first rib compared to the contralateral side; furthermore, sclerosis of the manubrium sterni. (b)CT image. In addition to increased sclerosis, small erosions can be identified in the sternocostal joint (arrow).
While the imaging findings are quite specific, they are not pathognomonic. Diagnosis is hampered in the absence of characteristic skin changes; these may have manifested several years previously.
Avascular necrosis (osteonecrosis) of the clavicle.
Malignant bone tumors:
Osteosarcoma.
Ewing sarcoma.
Metastasis.
At times, biopsy cannot be avoided for diagnosis confirmation.1
13.3 Tumors of the Chest Wall
The tumors described below are not specific to the chest wall but rather can occur anywhere in the entire musculoskeletal system. A guide to differentiate frequent benign from malignant tumors is given in ▶Table 13.1.
13.3.1 Benign Tumors
Benign tumors of the chest wall often exhibit characteristic imaging findings as presented in ▶Table 13.2. Typically, they are slowly growing and mostly asymptomatic. In particular, unlike the malignant tumors described in the following section, they do not cause pain of any significance.
Lipomas (see ▶Fig. 13.3) appear homogeneously fatty on CT and MRI. They occur in the chest wall both intramuscular and in the subcutaneous fat. In the latter setting, it is sometimes hardly possible to identify them on imaging despite evident clinical findings.
Fibrous dysplasia is monostotic in three-quarters of cases and polyostotic in one-quarter (see ▶Fig. 13.4). There is fusiform bulging and deformation of the affected bones, usually a rib, less commonly the clavicle. Amorphous calcifications are often observed on CT.3
Table 13.1 Benign and malignant tumors of the chest wall
Benign bone tumors: fibrous dysplasia, osteochondroma, aneurysmal bone cyst, giant cell tumor
Soft-tissue sarcomas
Chondrosarcoma
Osteosarcoma
Ewing sarcoma
Lymphomas
Myeloma
Malignant fibrous histiocytoma
Malignant nerve sheath tumors
Aggressive fibromatosis
Metastasis
Osteochondroma, a relatively common benign bone tumor, has a characteristic pedicled bony prominence (see ▶Fig. 13.5). The cartilage cap is best visualized on MRI; when the osteochondroma is oriented intrathoracically, it can also be seen on CT as a bony overlay of soft-tissue density.
Aneurysmal bone cysts are usually found in young adults. Their predilection sites in the chest wall are the posterior vertebral structures of the thoracic spine. Imaging demonstrates expansive osteolysis with cortical thinning.3
Giant cell tumors also occur in the same age group, affecting especially the sternum, clavicles, and ribs. Eccentric expansive osteolysis with cortical thinning is seen on imaging. Fluid-fluid levels are less common than in aneurysmal bone cysts.3
Table 13.2 Guide to differential diagnosis of benign tumors of the chest wall3
Fig. 13.3 Lipoma of the chest wall (arrow).CT image.
13.3.2 Malignant Tumors
Some malignant soft-tissue and bone tumors exhibit characteristic imaging findings, thus narrowing differential diagnosis (▶Table 13.3). A specific diagnosis of soft-tissue tumors, in particular, can usually only be made through invasive biopsy. However, in many cases imaging allows for differentiation from benign tumors.
Note
Unlike benign, generally asymptomatic, tumors, malignant tumors usually manifest clinically through pain.
Chondrosarcomas, the most common malignant bone tumors of the chest wall, have two age peaks (20 and over 50 years). A characteristic feature, which, however, is not always present, are the chondroid matrix calcifications identifiable especially on CT (see ▶Fig. 13.7). The tumors exhibit heterogeneous, in particular peripheral, contrast enhancement.4
Only gold members can continue reading. Log In or Register to continue