(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Esophageal Lesions
Mechanical Obstruction
Diagnosis
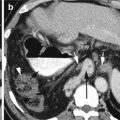
Achalasia
Imaging Features
1.
Dilated atonic esophagus filled with fluid and debris
2.
Lack of normal peristalsis
3.
Incomplete relaxation of the lower esophageal sphincter
4.
Bird-beak sign
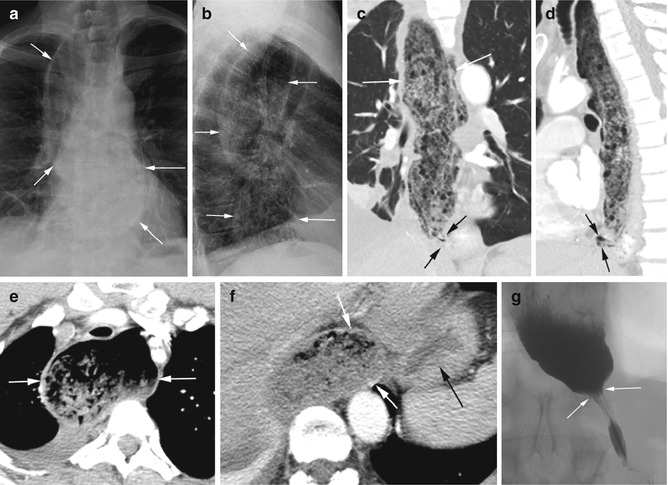
Fig. 15.1
Achalasia. (a, b) Chest x-ray PA and lateral views show debris-filled dilated esophagus (arrows). CT (c) coronal and (d) sagittal reformatted images show dilated debris-filled esophagus (white arrows) and narrowing at the GE junction (black arrows). Axial CT (e) shows dilated esophagus at the thoracic inlet (arrows) and (f) at the GE junction (white arrows) with collapse of the stomach (black arrows). (g) Barium swallow study shows bird-beak sign (arrows) with normal striation of mucosa at the gastroesophageal junction
Diagnosis
Boerhaave’s Syndrome
Imaging Features
1.
Periesophageal air collection in the distal esophagus from perforation
2.
Gas tracking into the left subphrenic and gastrohepatic spaces
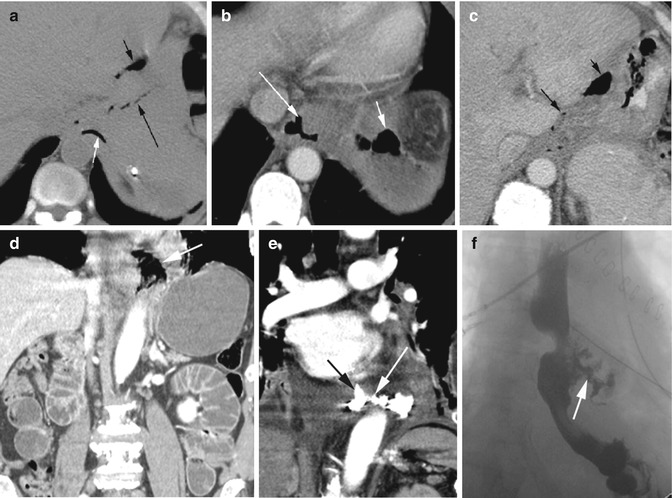
Fig. 15.2
Boerhaave’s syndrome. History of vomiting and upper abdominal pain in two patients. Patient 1: CT axial (a) noncontrast study shows air tracking from the distal esophagus (white arrow), surrounding the GE junction (long black arrow), and in the gastrohepatic space (short black arrow). (b, c) Axial CECT shows extraluminal gas around the esophagus (long white arrow) and gas in the left subphrenic space (short white arrow), around the GE region (long black arrow) and gastrohepatic space (short black arrow). Patient 2: (d) coronal reformatted CT shows collection of gas in the left side of the distal esophagus (arrow). The upper abdomen shows small bowel obstruction with dilated loops. (e) Coronal reformatted CT shows spillage of enteric contrast in the previous region of gas collection (arrow). (f) Barium swallow study shows rupture of the esophagus with contrast spillage from the distal esophagus (arrow)
Candida Esophagitis
Imaging Features
1.
Barium swallow study shows very irregular and shaggy appearance of the esophagus.
2.
Ulcerations filled with enteric contrast.
3.
CT shows diffusely thick enhancing mucosa and submucosal edema.
4.
Gas tracking into the submucosa.

Fig. 15.3
Candida esophagitis. Esophageal swallow study (a) shows lobulated contour of the esophageal mucosa from ulceration filled with contrast (black arrows). (b) Large abscess (long white arrows) with air-fluid level (short white arrows) in the right perihilar region from the tracheoesophageal fistula and multiple adjacent contrast-filled bronchi (short black arrows). (c) Axial CECT shows cobblestone appearance of the mucosa (thick black arrow) from coalescence of plaques and submucosal edema (thin black arrow). (d, e) Coronal and sagittal reformatted images again show thick mucosa (white arrow), submucosal edema, and speckled gas in the wall (black arrow) from ulcerations. (f) Axial CT shows large abscess in the right paravertebral region (white arrows) tracking from the esophagus (black arrow)
Malignancies
Diagnosis
Squamous Cell Carcinoma
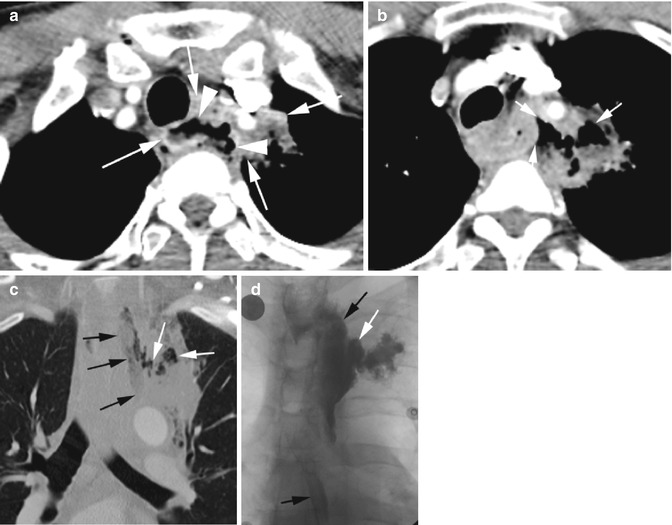
Fig. 15.4
Esophageal squamous cell carcinoma in the superior mediastinum. Axial CECT (a) shows a large soft tissue mass around the esophagus in the superior mediastinum extending to the left upper lobe (LUL) (white arrows) with irregular mucosal surface (arrowheads). (b) At a lower level, a large gas collection is seen extending from the esophagus to the mass in the LUL (arrows). (c) Coronal reformatted image again shows gas tracking from the esophagus (black arrows) to mass in the LUL (white arrows). (d) Esophageal swallow study shows extravasated contrast (white arrow) from the esophagus (black arrow) into the LUL
Diagnosis
Carcinoma at the Carina with Tracheoesophageal Fistula
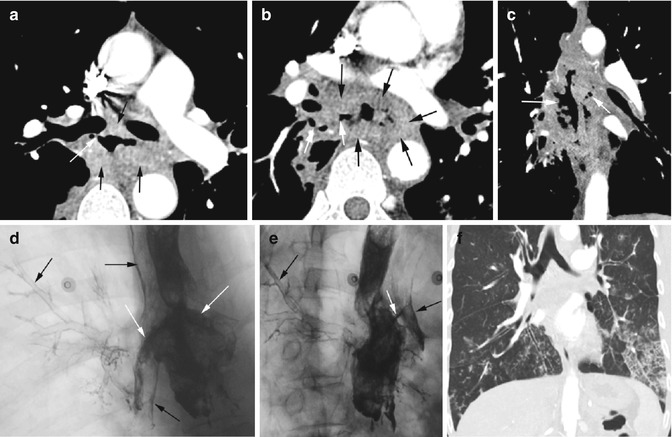
Fig. 15.5
Esophageal carcinoma at the carina with tracheoesophageal fistula. CT axial (a, b) shows a large soft tissue mass around the esophagus (black arrows). Fistula with gas is tracking to the right main stem and lower lobe bronchus (white arrow). (c) Coronal reformatted CT shows gas tracking on either side of the esophagus (white arrows). Esophageal swallow study (d, e) shows contrast spilling into main stem bronchi bilaterally (white arrows) with contrast lining the trachea and right middle lobe and lower lobe bronchi (black arrows). (f) Coronal reformatted CT of the chest after the swallow study shows aspiration mainly in the lung bases with bronchocentric nodules and ground-glass infiltrates
Diagnosis
Adenocarcinoma with Perforation
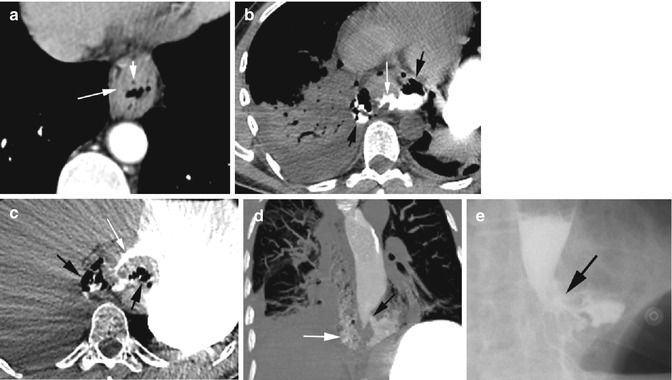
Fig. 15.6
Adenocarcinoma of the distal esophagus with perforation. (a) Axial CECT shows wall thickening of the esophagus (long arrow) with multiple small perforated gas (short arrow) within the tumor. (b, c) Noncontrast axial CT 1 month later shows irregular narrowing of the esophagus lumen (white arrow) and perforation with periesophageal gas and enteric contrast medially and laterally (black arrows). (d) Coronal reformatted image and esophageal swallow study (e) show contrast spillage out of the distal esophagus (black arrow). The CT shows gas and contrast tracking up in the mediastinum (white arrow)
Diagnosis
Stricture
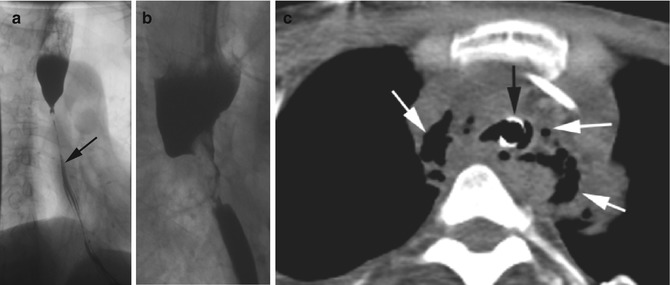
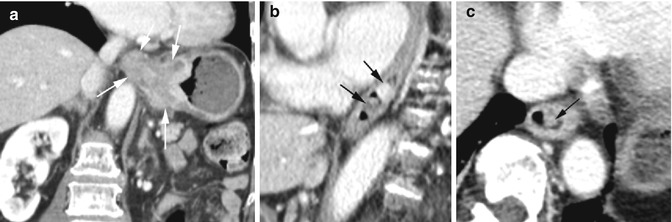
Fig. 15.7
Esophageal stricture of three patients. (a) Esophageal swallow study shows smooth long segment of narrowing of the esophagus (arrow) from the level of the arch of the aorta. History of lye ingestion. (b) Barium swallow study shows a short segment of irregular narrowing of the esophagus from squamous cell carcinoma. (c) Axial CT shows perforation of the esophagus in the superior mediastinum with extraluminal gas (white arrows). Endotracheal tube in the trachea (black arrow). History of cocaine swallow with odynophagia. Endoscopic examination showed stricture from squamous cell carcinoma
Fig. 15.8
Adenocarcinoma at the gastroesophageal junction as polypoid growth within the esophageal lumen. CECT coronal reformatted image (a) shows a large mass at the GE junction (arrows). Sagittal reformatted (b) and axial images (c) show two small polypoid protrusions within the esophageal lumen (arrows)
Diagnosis
Leiomyosarcoma
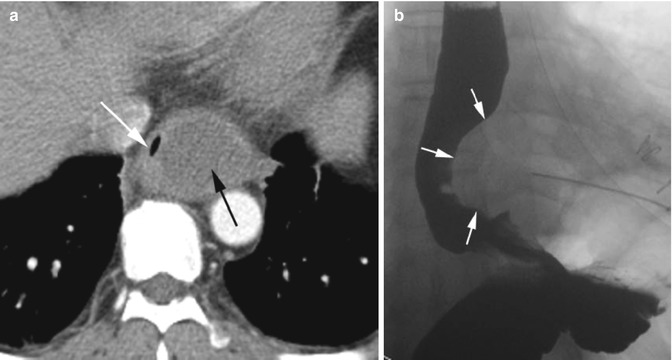
Fig. 15.9
Leiomyosarcoma of the esophagus, biopsy proven. Axial CT (a) image shows a large low-density intramural mass in the lower esophagus (black arrow) causing extrinsic compression of the esophageal lumen (white arrow). (b) Barium swallow study shows extrinsic compression of the distal esophagus by mass (white arrows)
Non-malignant Bowel Lesions
Mechanical Bowel Obstruction
Diagnosis
Organoaxial Gastric Volvulus
Imaging Features
1.
The stomach has herniated through esophageal hiatus.
2.
Twisting of the stomach along its long axis with the greater curvature superiorly positioned.
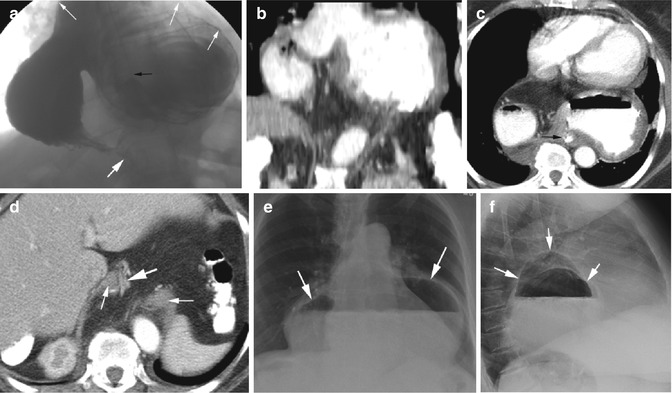
Fig. 15.10
Organoaxial volvulus. (a) Barium swallow study shows dilated stomach in the mediastinum with the greater curvature superiorly positioned (thin white arrows). Small amount of enteric contrast in the duodenum (thick white arrow). Nasogastric tube is seen in the distal esophagus (black arrow). (b) CT coronal reformatted image shows a similar position of the stomach as in the swallow study. (c) Axial CT shows nasogastric tube in the distal esophagus (arrow) with the twisted stomach anterior to it. (d) Axial CT shows the two ends of the diaphragm (thin white arrows) of the wide esophageal hiatus and duodenum (thick white arrow) entering the abdomen. (e, f) Chest x-ray PA and lateral views show large hiatus hernia in the posterior mediastinum (arrows)
Diagnosis
Mesenteroaxial Volvulus
Imaging Features
1.
Transverse folding of the stomach with its distal end herniating through the hiatus into the thorax.
2.
The fundus of the stomach and gastroesophageal junction is below the diaphragm.
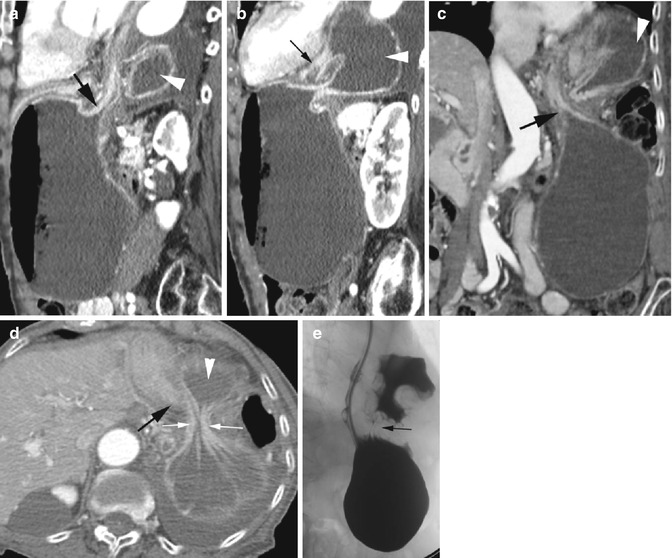
Fig. 15.11
Mesenteroaxial volvulus. CT sagittal (a, b) and coronal (c) reformatted images and axial (d) images show the fundus of the stomach with the GE junction (thick black arrow) below the diaphragm. The distal end of the stomach (arrowhead) has herniated through the narrow esophageal hiatus (thin white arrows in d) into the thorax. The duodenum is seen doubling back into the abdomen (thin black arrow b). (e) Barium swallow study again shows nasogastric tube entering the stomach below the diaphragm with the distal body of the stomach above the diaphragm and is constricted at the hiatus (arrow)
Diagnosis
Sigmoid Volvulus
Imaging Features
1.
Redundant sigmoid colon
2.
Coffee bean sign in supine radiograph
3.
Proximal and distal ends twist in the pelvis, bird-beak sign
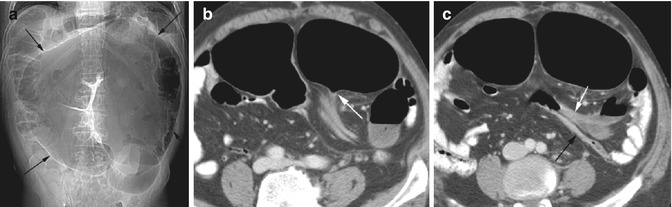
Fig. 15.12
Sigmoid volvulus. (a) Supine radiograph shows the coffee bean sign of the sigmoid volvulus (arrows). Axial CT (b) shows the beak of the twisted end of the sigmoid loop (arrow) and (c) shows the two collapsed ends that twist (arrows)
Diagnosis
Cecal Volvulus
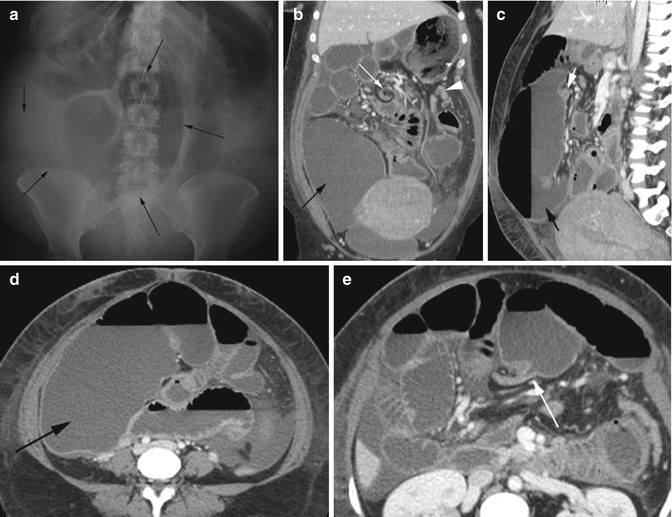
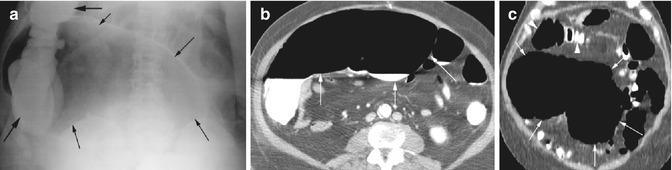
Fig. 15.13
Cecal volvulus. (a) Supine radiograph shows markedly a dilated cecum (arrows) in the lower abdomen with dilated small bowel loops. CT (b) coronal and (c) sagittal reformatted images show a markedly distended cecum (black arrow), ascending colon, and small bowel loops. The distal ascending colon is seen to be constricted due to twisting (white arrow), and the rest of the colon is collapsed (arrowhead). Axial CT (d) shows a markedly dilated right colon (arrow), and (e) shows the transition end which is collapsed with bird-beak sign (arrow). Patchy necrosis was seen in the cecum at surgery and the small bowel mesentery was found not to be tethered to the retroperitoneum
Fig. 15.14
Cecal bascule. (a) Supine AP radiograph of the abdomen shows dilated cecum (thin arrows) which is displaced medially. Barium enema contrast is seen in the distal right colon (thick arrows). CT (b) axial and (c) coronal reformatted images again show the dilated cecum folded and medially displaced (white arrows). The rest of the colon (arrowheads) is not dilated
Diagnosis
Transverse Colon Volvulus
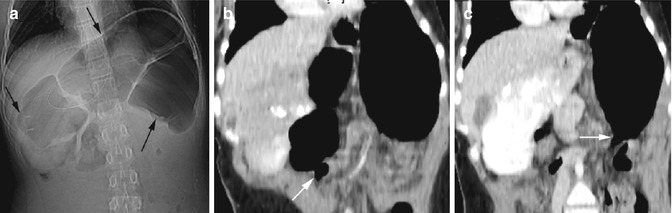
Fig. 15.15
Volvulus of the transverse colon. (a) Supine radiograph of the abdomen shows dilatation of the transverse colon (arrows). CT (b, c) coronal reformatted images show dilated transverse colon with narrowing at the hepatic and splenic flexures (arrows). At surgery, the transverse mesocolon was seen to be absent which was repaired. Patient had intermittent upper abdominal pain from folding of the transverse colon over the fixed points of the hepatic and splenic flexures
Diagnosis
Small Bowel Volvulus
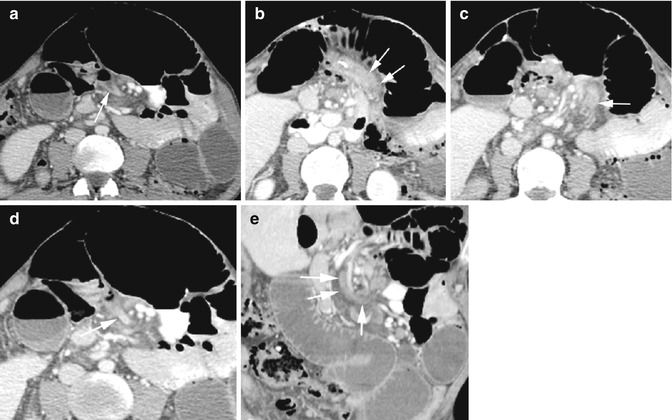
Fig. 15.16
Small bowel volvulus. CT axial (a–d) and coronal reformatted (e) shows twisting (arrows) of a loop of the small bowel around the superior mesenteric vessels with dilatation of the loops proximally. The twisting loop is constricted
Closed-Loop Obstruction
Diagnosis
Small Bowel Closed-Loop Obstruction
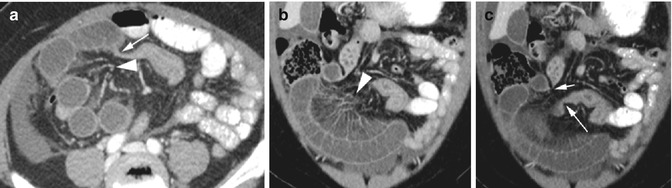
Fig. 15.17
Closed-loop small bowel obstruction from adhesion by a piece of the omentum. CT (a) axial and (b) coronal reformatted images show dilated loops of the small bowel in the right abdomen with the mesenteric blood vessels converging to a point (arrowhead). A transition point is seen (thin white arrow). (c) Coronal reformatted image at a different plane shows the two constricted ends of the closed-loop small bowel obstruction (short and long arrows)
Diagnosis
Large Bowel Closed-Loop Obstruction
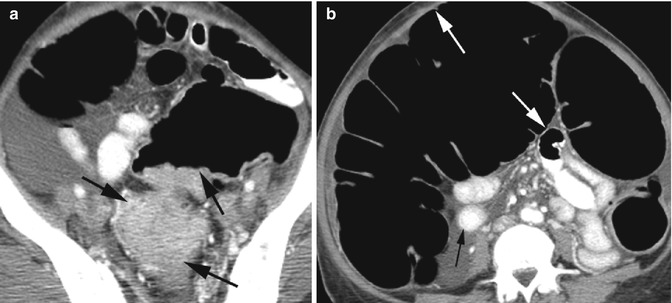
Fig. 15.18
Closed-loop obstruction of the colon by tumor and a competent ileocecal valve. Axial CT (a) shows a large mass obstructing the distal sigmoid colon. (b) The cecum which is medially deviated is dilated (white arrows) more than 12 cm due to a competent ileocecal valve. The small bowel loops are of normal caliber (black arrow)
Diagnosis
Afferent Loop Syndrome
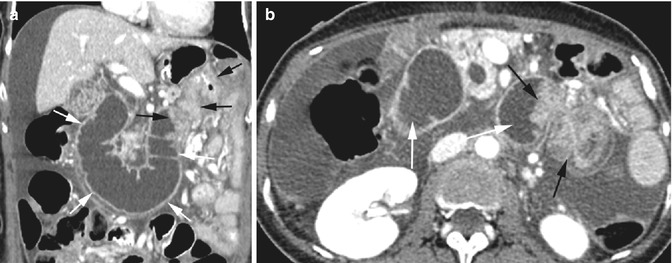
Fig. 15.19
Afferent loop syndrome. History of gastric carcinoma with Billroth II anastomosis. CT (a) coronal reformatted and axial (b) images show dilated fluid-filled duodenum (white arrows). The anastomosis site of the duodenojejunal junction is obstructed by enhancing soft tissue mass due to tumor recurrence (black arrows)
Hernia
Diagnosis
Left Paraduodenal Internal Hernia
Imaging Features
1.
Encapsulated group of small bowel loops.
2.
Located between the stomach and pancreas.
3.
Mesenteric vessels supplying the herniated bowel loops are crowded and stretched within the hernia and constricted at the neck of the hernia.
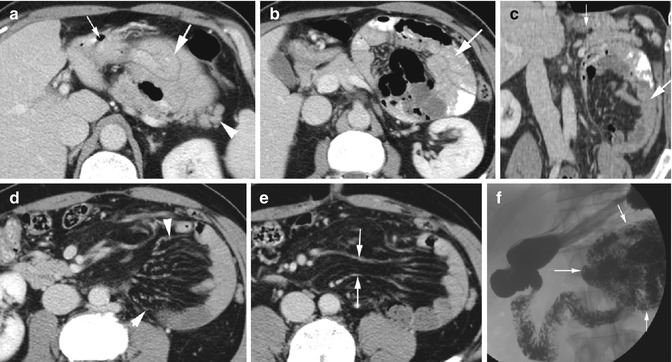
Fig. 15.20
Paraduodenal internal hernia. CT axial (a, b) and coronal reformatted images (c) show a cluster of the small bowel in the shape of a cocoon (thick white arrow) between the stomach (thin white arrow) and pancreas (arrowhead). Axial CT (d) shows crowding of the mesenteric vessels to the herniated loops (arrowheads). (e) The vessels at the neck of the hernia are stretched and constricted (arrow). (f) Barium swallow study shows clustered small bowel loops adjacent to the duodenojejunal junction (arrows)
Diagnosis
Internal Herniation into the Pelvis

Fig. 15.21
Internal herniation into the pelvis. Axial CT (a, b) shows a large hemorrhagic ovarian cyst (white arrows) with dilated obstructed small bowel loops (black arrows) posterior to the uterus (thick black arrow). At surgery, the hemorrhagic cyst was adherent to the sigmoid colon and the sigmoid mesentery, and the small bowel had herniated through an opening in the adhesion
Diagnosis
Inguinoscrotal Hernia
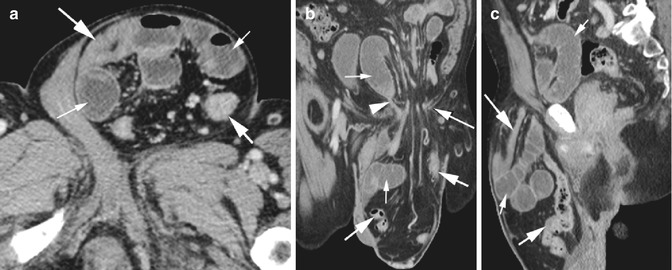
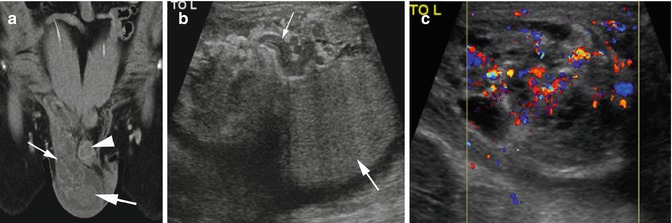
Fig. 15.22
Scrotal herniation of the small bowel with obstruction. CT axial (a), coronal (b), and sagittal (c) reformatted images show herniation of the small and large bowel loops through the left inguinal ring into the scrotum with obstruction of a small bowel loop (arrowhead) at the inguinal ring (long thin arrow). The herniated colon (short thick arrow) and some small bowel loops (long white arrow) are collapsed. The obstructed small bowel loops are dilated (thin arrow) in the hernia and in the abdomen
Fig. 15.23
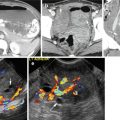
Bowel herniation into the scrotum with no obstruction. (a) CT coronal reformatted image shows bowel loops in the right inguinal canal (thin arrow) extending to the scrotum up to the Testis (thick arrow) on the right side of the penis (arrowhead). (b) Grayscale ultrasound image shows fluid-filled bowel loops (thin arrow) anterior to the testes (thick arrow). (c) Color Doppler shows patency of the mesenteric vessels
Diagnosis
Incisional Hernia with Infarction
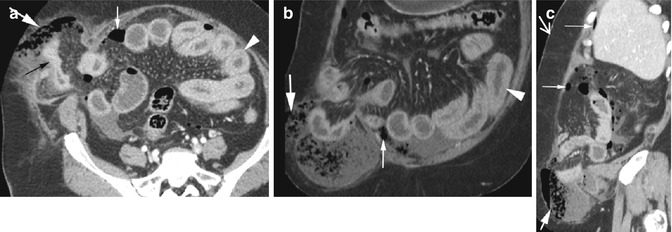
Fig. 15.24
Incisional hernia with infarction. CT axial (a), coronal (b), and sagittal (c) reformatted images show herniation of small bowel loops (black arrow) through right abdominal wall defect. The herniated loop is collapsed due to perforation but shows enhancement indicating that arterial supply is patent. Gas collection is seen in the herniated sac (thick white arrow) which is spilling into the peritoneal cavity (thin white arrow). Acute ischemic changes with wall thickening are seen in some intra-abdominal small bowel loops (arrowhead) and with mesenteric vascular engorgement
Diagnosis
Obstructed Abdominal Wall Hernia
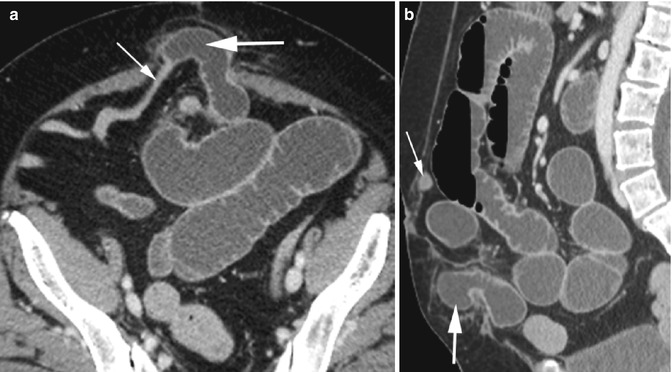
Fig. 15.25
Abdominal wall hernia with small bowel obstruction. CT axial (a) and sagittal reformatted (b) images show obstruction of herniated small bowel loop through infraumbilical abdominal wall defect. The afferent loop (thick arrow) is dilated with collapse of the efferent loop (thin arrow)
Diagnosis
Richter Hernia
Imaging Features
1.
Herniation of the antimesenteric wall of a bowel loop through the anterior abdominal wall.
2.
Does not cause bowel obstruction.
3.
It can become necrotic and can perforate.
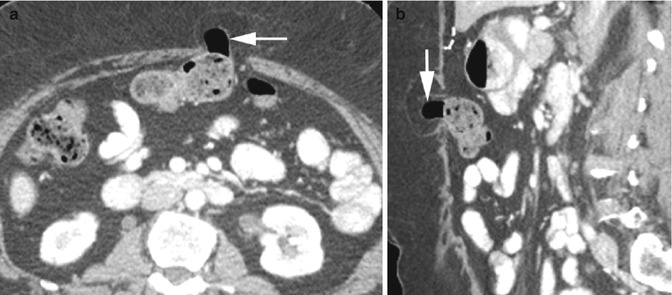
Fig. 15.26
Richter hernia. CT axial (a) sagittal reformatted (b) images show protrusion of the antimesenteric wall of the transverse colon (arrow) through anterior abdominal wall defect
Bowel Stricture
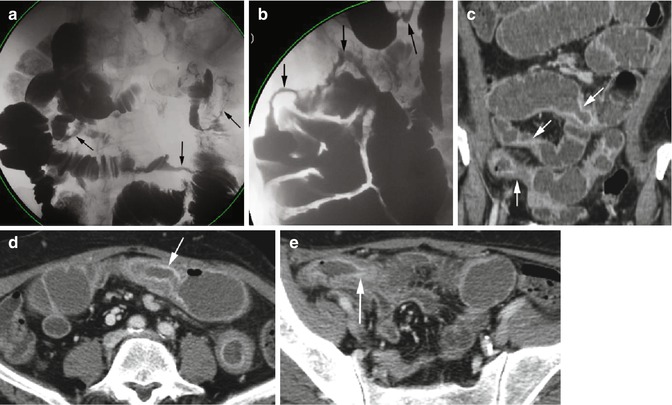
Fig. 15.27
Small bowel obstruction from multiple strictures. A patient with cytomegalovirus enteritis had balloon enteroscopy which showed multiple ulcers and strictures in the jejunum. Barium swallow study (a, b) shows multiple strictures in small bowel loops (arrows). CT coronal reformatted (c) and axial views (d, e) show small bowel obstruction with multiple focal strictures with wall thickening (arrows) at stricture sites
Intussusception
Diagnosis
Rectosigmoid Intussusception
Imaging Features
1.
Multilayered or bowel within bowel appearance of affected bowel loop.
2.
The intussusceptum with its surrounding blood vessels and mesenteric fat is surrounded by the intussuscipiens.
3.
May or may not have lead points.
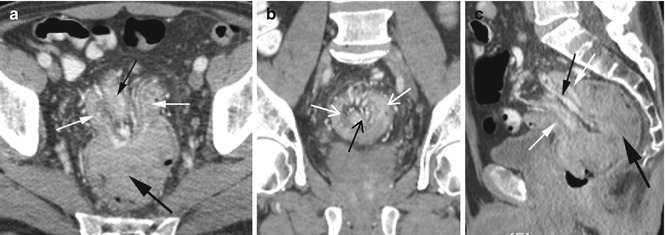
Fig. 15.28
Rectosigmoid intussusception with adenocarcinoma of the rectum as the lead point. CT axial (a), coronal (b), and sagittal (c) reformatted images show a large solid mass (thick black arrow) dragging the intussusceptum with its surrounding vessels and fatty tissue (black arrow) through the intussuscipiens (white arrows)
Diagnosis
Ileocolic Intussusception
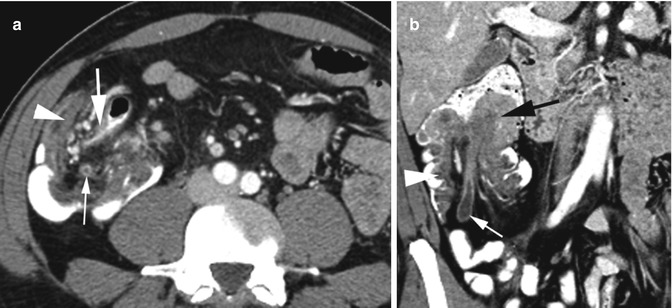
Fig. 15.29
Ileocolic intussusception with tubulovillous adenoma as lead point. CT axial (a) shows intussusceptum composed of the terminal ileum (thick white arrow), appendix (thin white arrow), and surrounding mesenteric vessels and adipose tissue within the cecum (arrowhead) which is the intussuscipiens. (b) Coronal reformatted image shows soft tissue mass (black arrow) at the tip of the intussusceptum with the appendix and mesenteric vessels and fat (thin white arrow) behind it and surrounded by the ascending colon as intussuscipiens (arrowhead)
Diagnosis
Colocolic Intussusception
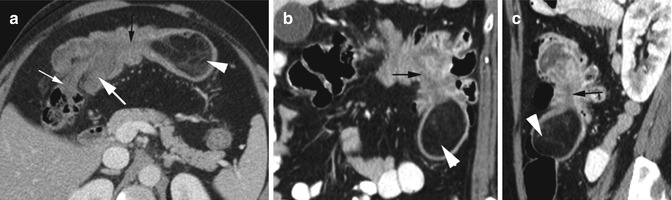
Fig. 15.30
Colocolic intussusception with lipoma as lead point in two patients. CT axial (a) view shows the proximal transverse colon as intussusceptum (thin white arrow) surrounded by mid-transverse colon as intussuscipiens (thick white arrow). The lipoma (arrowhead) at the distal end has a long thin pedicle (black arrow) traversing the intussuscipiens. CT coronal (b) and sagittal (c) reformatted views in the second patient show lipoma (arrowhead) as the lead point of the intussusceptum with long pedicle (black arrow) in the splenic flexure
Diagnosis
Jejunal Intussusception
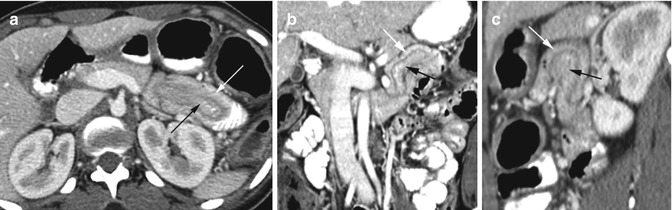
Fig. 15.31
Intussusception of the proximal jejunum with no lead point. CT axial (a), coronal (b), and sagittal (c) reformatted images show the intussusceptum (black arrow) surrounded by a halo of adipose tissue within the intussuscipiens (white arrow)
Gastric Outlet Obstruction
Imaging Features
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


