(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Urinary Stones
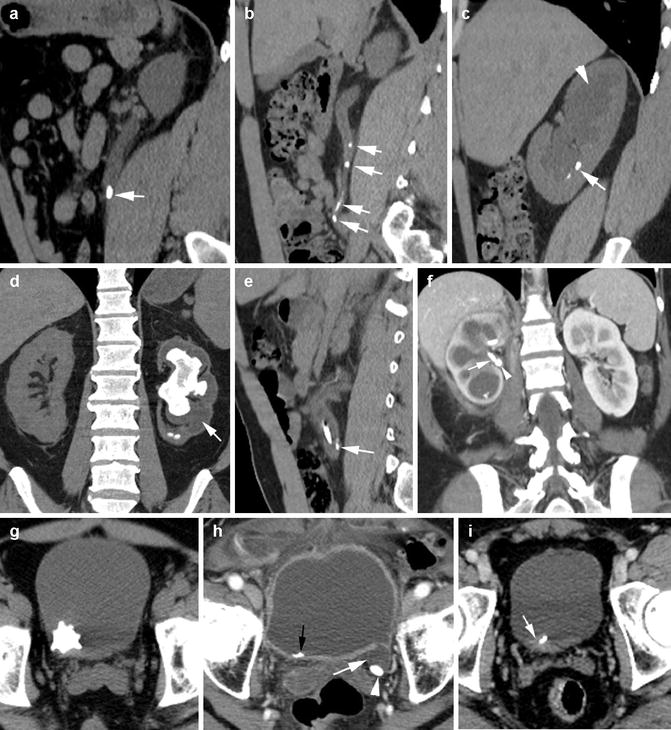
Fig. 14.1
Urinary stones in different patients. Noncontrast sagittal reformatted CT (a) shows a single stone (arrow) in the ureter which is dilated proximal to the stone. (b, c) Multiple stones in the right ureter (arrows) with hydronephrosis (arrowhead) and stones in lower pole calyces (arrow). (d) Coronal reformatted image shows large staghorn stone in the left kidney with hydronephrosis. The calyces distal to the stone are dilated and fluid filled (arrow). (e) Sagittal reformatted image shows stone (arrow) along with stent and hydroureter. (f) Postcontrast coronal reformatted image shows a stone (arrowhead) with stent (white arrow) at UPJ causing hydronephrosis. Axial CT (g) shows a jackstone urinary bladder. Axial CT shows (h) a stone (arrowhead) in Hutch diverticulum (white arrow) and a small stone within the bladder (black arrow). (i) Stone at ureterovesical junction with surrounding soft tissue (arrow) of the bladder wall
Urinoma
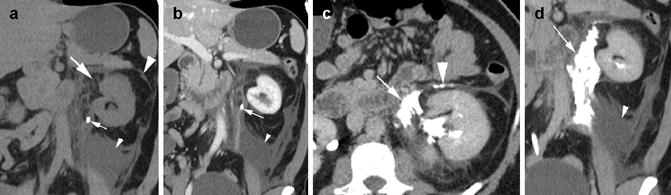
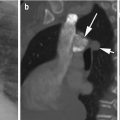
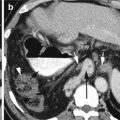
Fig. 14.2
Urinoma from ureteral stone. CT coronal reformatted images in precontrast (a) and arterial phase (b) show a stone (thin arrow) in the proximal ureter with stranding in the perirenal space medially (thick arrow), large fluid collection (small arrowhead) in the inferior perirenal cone-shaped space, and thick anterior renal fascia (thick arrowhead). Excretory phase, axial CT (c), and coronal reformatted (d) images show contrast in the perirenal space (thin arrow), in the anterior interfascial space (thick arrowhead), and extending inferiorly around the ureter (arrow in d)
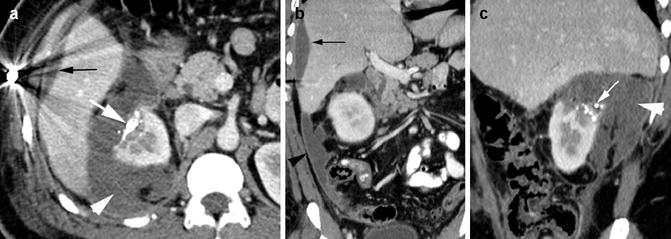
Fig. 14.3
Urinoma post gunshot injury and renal embolization. Postcontrast axial CT (a), coronal (b), and sagittal (c) reformatted images show truncated right kidney upper pole from GSW. Radio-opaque densities in the upper pole are from glue (thick white arrow) used to embolize the pseudoaneurysms of the renal artery branches. A large fluid (arrowhead) which was tested to be urine surrounds the upper pole of the kidney and is spilling into the peritoneal cavity. The peritoneum shows mild thickening from reactive changes (black arrowhead). Fluid in subcapsular region at the right lobe of the liver (black arrow) is due to resolving hematoma from liver laceration
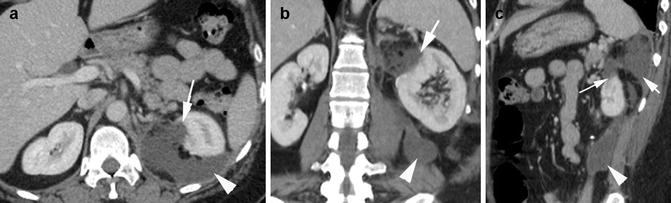
Fig. 14.4
Urinoma or chyle. Old resection of the upper pole of the left kidney for MRSA abscess. Postcontrast CT, axial (a), coronal (b), and sagittal (c) reformatted images show deformity of the upper pole of the left kidney with fluid extending from the defect (long arrow) to the perirenal space and then to the posterior (arrowhead) and anterior pararenal (short arrow) spaces
Tubulointerstitial Nephritis
Diagnosis
Bacterial Pyelonephritis
Imaging Features:
1.
Renal enlargement
2.
Striated nephrogram with one or multiple wedge-shaped areas of decreased enhancement involving the cortex
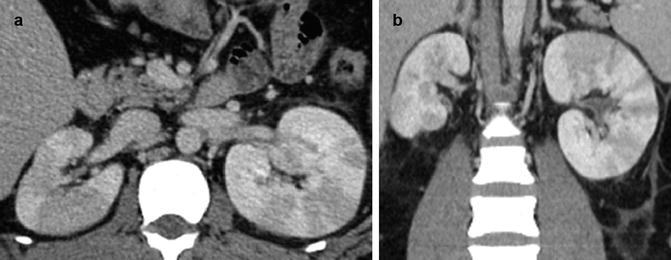
Fig. 14.5
Bacterial pyelonephritis. (a) Postcontrast axial CT and coronal reformatted CT images (b) show bilateral renal low-density striations
Diagnosis
Postobstructive Striated Nephrogram
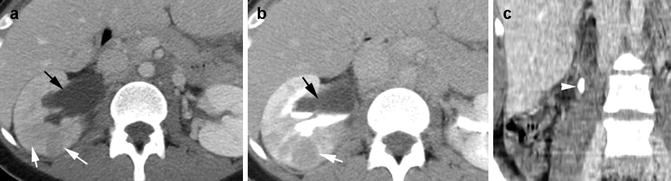
Fig. 14.6
Postobstructive striated nephrogram. No systemic or urinary infection. Postcontrast axial CT in nephrographic phase (a), delayed excretory phase CT (b), and coronal reformatted images (c) show hydronephrosis of the right kidney (black arrow) with renal parenchymal striations (white arrows). Large stone is seen in the proximal right ureter (arrowhead)
Diagnosis
Sarcoidosis
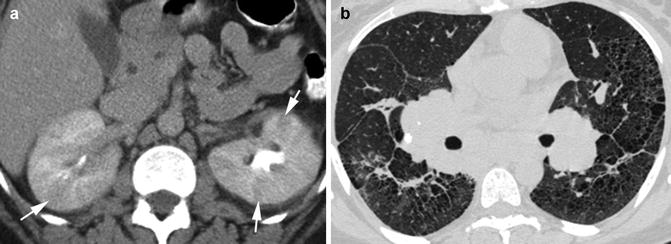
Fig. 14.7
Sarcoidosis. Postcontrast axial CT (a) shows multiple linear hypoattenuating striations (arrows) in both kidneys related to sarcoidosis with no clinical evidence of infection. (b) Chest of the same patients shows bilateral hilar lymphadenopathy and interstitial fibrotic changes
Diagnosis
Tumor Lysis Syndrome
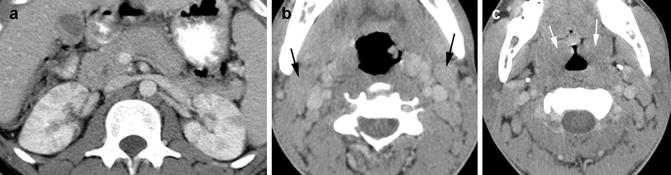
Fig. 14.8
Tumor lysis syndrome. Patient with Burkitt’s lymphoma on chemotherapy. Axial CT (a) of the kidneys shows multiple focal striations from acute kidney injury with no evidence of infection. (b, c) CT of the neck shows enlarged lymph nodes (black arrows) and palatine tonsils (white arrows)
Diagnosis
Allergic Nephritis
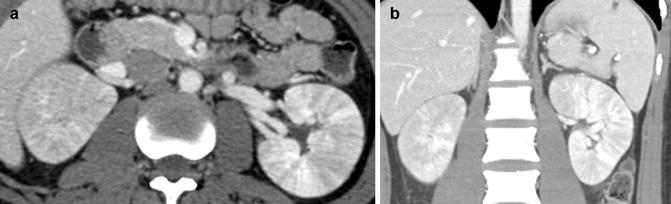
Fig. 14.9
Acute interstitial (allergic) nephritis. Patient with ALL on methotrexate. Postcontrast axial (a) and coronal reformatted (b) CTs show diffuse low-attenuated renal striation bilaterally
Diagnosis
Acute Kidney Injury
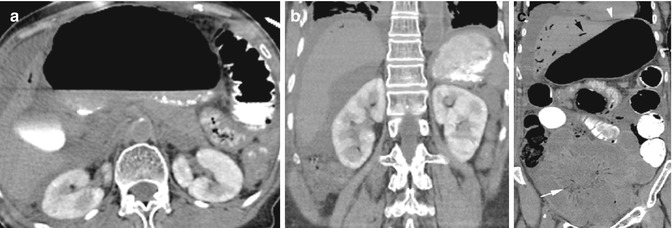
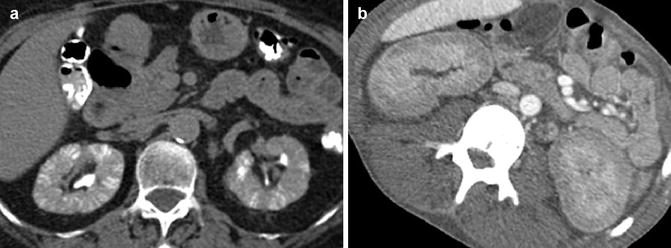
Fig. 14.10
Acute kidney injury with diffuse ischemic changes in bowels. (a) Noncontrast axial CT and (b, c) coronal reformatted image show retained contrast in renal cortex from CECT done the previous day. Bowel loops are dilated with gas in mesenteric veins (white arrow), portal veins (black arrow), and small pneumoperitoneum (arrowhead)
Fig. 14.11
Acute kidney injury. Patient 1: Axial CT (a) unenhanced study shows dense striations involving both the cortex and medulla in both kidneys from retained contrast in tubules. Patient soon recovered. Patient 2: (b) History of shortness of breath in a 30-year-old male with AIDS and end-stage renal disease. Postcontrast CT shows cortical necrosis with contrast only in the medullary portion of the kidneys
Diagnosis
Renal Infarction
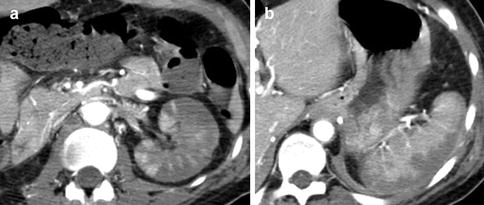
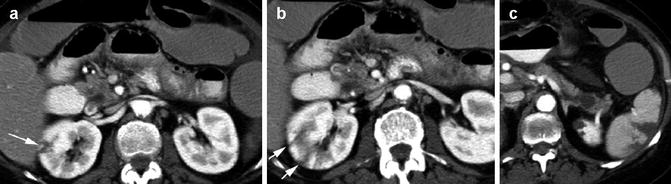
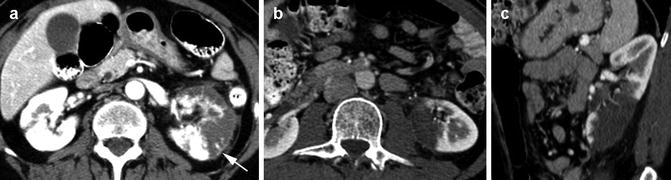
Fig. 14.12
Renal infarction. Patient with Takayasu arteritis with stenosis of the left renal artery. Postcontrast axial CT (a) shows multifocal, patchy wedge-shaped areas of decreased attenuation involving both the cortex and medulla involving the capsular surface. (b) Axial CT shows infarction of periphery of the spleen
Fig. 14.13
Focal renal infarction in SLE. Axial CT images show (a, b) multifocal striated infarction of the right kidney (arrows) which were absent 10 days prior. (c) Infarction of lateral border of the spleen. Diffuse dilated bowel loops were found to be necrotic
Fig. 14.14
Lobar renal infarction. Patient 1: (a) History of atrial fibrillation. Axial CT shows small focal infarction of the right kidney and large infarction of the left kidney with cortical rim sign (arrow). Patient 2: (b, c) History of marijuana use and sudden back pain with moderate heavy lifting. Axial and coronal CTs show large area of infarction at the lower pole of the left kidney
Nephritis
Diagnosis
Emphysematous Pyelitis
Imaging Features
1. Gas-fluid level in dilated calyces and ureters with no pyelonephritis
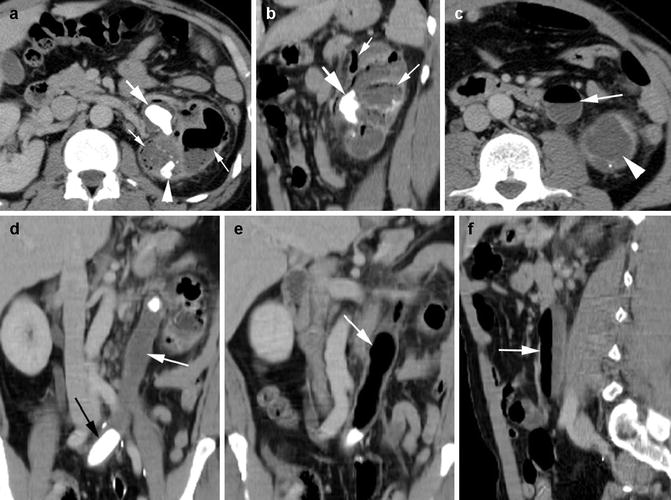
Fig. 14.15
Emphysematous pyelitis and ureteritis. History of bladder cancer, ileal conduit, left upper quadrant pain, and purulent discharge through left nephrostomy tube. CECT, axial (a), and sagittal reformatted (b) images show staghorn stone (thick arrow) in the renal pelvis and stone at the lower pole renal calyx (arrowhead). Emphysematous changes with fluid and gas in dilated calyces (thin arrow). Axial CT at lower level (c) shows gas and fluid in dilated left ureter (arrow) and fluid-filled lower pole left kidney (arrowhead). Coronal reformatted images (d, e) and sagittal reformatted image (f) show a second stone distal to the left ureter (black arrow) with air-fluid collection (thin arrow) in the ureter obstructed by the two stones
Diagnosis
Emphysematous Pyelonephritis
Imaging Features
1.
Parenchymal enlargement and destruction with gas collections
2.
Streaky or bubbly gas or gas-fluid level
3.
Focal tissue necrosis with or without abscess
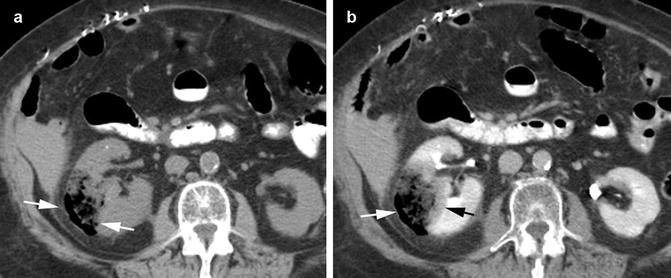
Fig. 14.16
Emphysematous pyelonephritis in an 82-year-old female. (a) Axial CT precontrast phase shows focal area of tissue necrosis midpole right kidney (arrows) with gas collection. (b) Postcontrast axial CT shows the gas to be contained within the capsule (white arrow). A thin rim of edema is seen surrounding the necrosis (black arrow). Urine culture grew E. coli
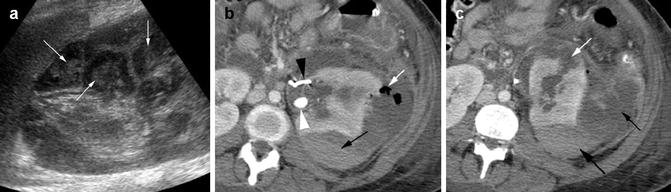
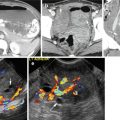
Fig. 14.17
Pyonephrosis with rupture. A pregnant 27-year-old patient with urosepsis. (a) US of the left kidney shows dilated calyces with debris (arrows). Patient had spontaneous abortion. CT done 5 days later. Axial CECT (b) shows a large stone in the renal pelvis (white arrowhead) with adjacent stent (black arrowhead). Gas bubbles extending into the subcapsular space from the renal parenchyma (white arrow) and also hematocrit level (black arrow). (c) Rupture of calyx into subcapsular space (white arrow) with fluid (thin black arrow) and hemorrhage (thick black arrow) in the subcapsular space. Patient had left nephrectomy, and urine grew Acinetobacter baumannii/haemolyticus
Diagnosis
Xanthogranulomatous Pyelonephritis
Imaging Features
1.
Large staghorn calculus in most cases
2.
Affected kidney is enlarged and nonfunctioning
3.
Contracted renal pelvis, expansion of renal calyces, and inflammatory changes in perinephric fat
4.
Extrarenal extension with formation of psoas abscess and fistula to the skin or colon
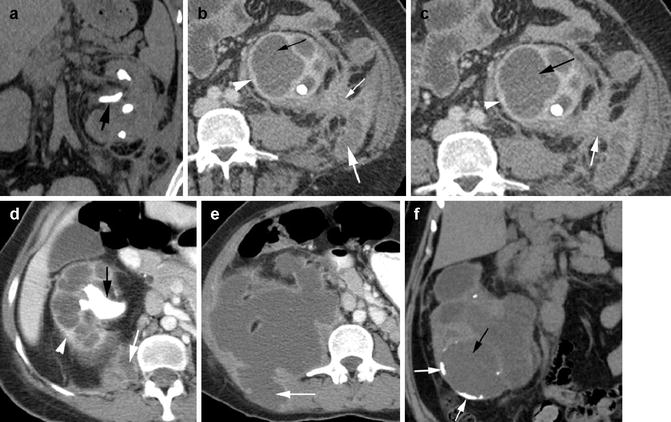
Fig. 14.18
Xanthogranulomatous pyelonephritis in three patients. Patient 1: (a) Noncontrast coronal reformatted (b, c) CECT shows enlarged left kidney with central staghorn stone (thick black arrow) and dilated calyces (thin black arrow). Inflammatory changes (thin white arrow) with fluid (thick white arrow) extend from the kidney to the peri- and pararenal spaces. Mild rim enhancement is seen of the calyces (arrowhead). Patient 2: CECT axial images (d, e) show enlarged right kidney with staghorn stone and dilated calyces with rim enhancement. A large collection of nonenhancing thick-rimmed fluid is extending from the lower pole of the kidney to the psoas muscle and posterior abdominal wall (arrow). Patient 3: (f) Coronal reformatted noncontrast CT shows dilated calyces (black arrow) with rim calcification (short white arrows)
Diagnosis
Abscess
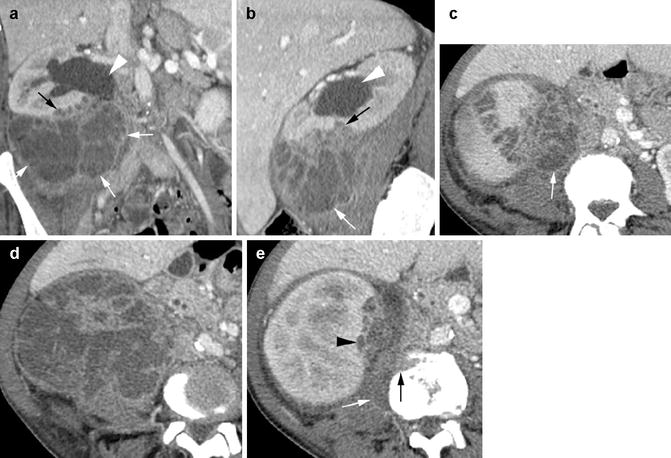
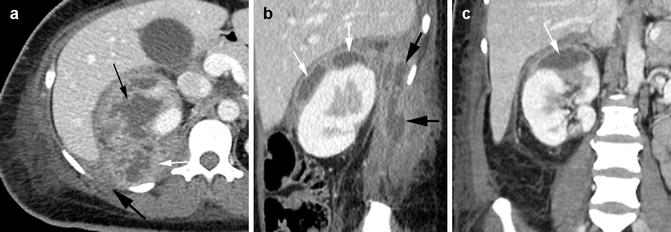
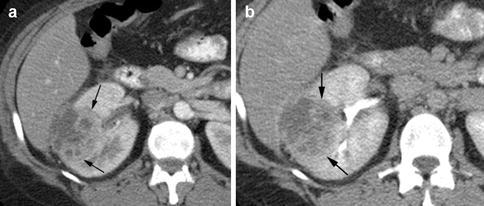
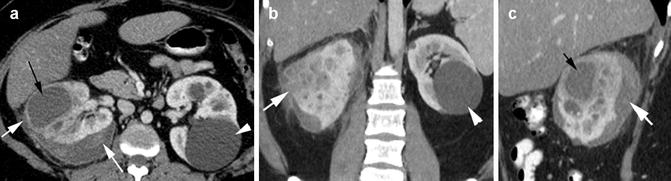

Fig. 14.19
Intrarenal abscess with perirenal extension and osteomyelitis. History of IV drug abuse and MRSA infection. CECT (a, b) coronal and sagittal reformatted images show multiple small abscesses in lower pole of the right renal parenchyma (black arrow) with large extension into perirenal space inferiorly (white arrows) and hydronephrosis (arrowhead) from obstruction of the ureter by the abscess. (c, d) Axial images show extension medially through the fascia muscularis (arrow) to the psoas muscle. (e) Axial CECT shows osteomyelitis of L3 vertebral body (black arrow) with paravertebral abscess (white arrow) from the lower pole abscess (arrowhead)
Fig. 14.20
Renal abscess extending to the posterior abdominal wall. CECT (a) axial, (b) sagittal, and (c) coronal reformatted images show parenchymal abscess (thin black arrow) in the upper pole of the right kidney is extending to the subcapsular and posterior pararenal space (thin white arrow) and then into the posterior abdominal wall (thick black arrow)
Fig. 14.21
Renal abscess compressing the liver. History of diabetes, fever, and hematuria. Axial postcontrast CT in (a) arterial (b) delayed phases show focal well-demarcated abscess with septations within the midpole of the right renal parenchyma (arrows) causing extrinsic compression on the liver
Fig. 14.22
Renal abscess involving the subcapsular space. Postcontrast CT (a) axial, (b) coronal, and (c) sagittal reformatted images show a large abscess of the right kidney (thin black arrow in a and c) and surrounding smaller abscesses (b) extending into the subcapsular space (white arrow) with edema of the surrounding renal parenchyma. Infected fluid collection is seen in the subcapsular space (thick white arrow), is of heterogeneous density causing extrinsic compression of the kidney, and was drained. The left kidney has a simple cyst (arrowhead)
Fig. 14.23




Multifocal abscess. History of diabetes. CECT (a) axial, (b) coronal, and (c) sagittal reformatted images show multiple abscesses mainly in the left kidney (black arrows). Pyelitis is seen of the renal pelvis with enhancement of the wall of the renal pelvis (white arrows)
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
