Lateral Elbow
Common Extensor Origin Epicondylalgia
The commonest cause of pain in the lateral aspect of the elbow is tendinopathy or enthesopathy of the common extensor origin (CEO). The term ‘tennis elbow’ originates from early descriptions of this condition and it has largely stuck, passing into common usage. Despite the name, the condition occurs much more commonly in nontennis players and a wide variety of occupations and sports have been implicated. It is more common in golfers than is golfer’s elbow (common flexor origin tendinopathy).
The characteristic location of pain is over the lateral epicondyle. The patients may also note muscle weakness, particularly in grip strength.
| Thompson’s manoeuvre: resisted wrist dorsiflexion with the elbow extended and the forearm pronated results in pain, which radiates down the forearm. |
The differential diagnosis of lateral side pain includes CEO tendinopathy, injuries to the radial collateral ligament (RCL) synovial plica, osteochondritis dissecans (OCD), radiocapitellar arthritis, radial tunnel syndrome, cervical radiculopathy and posterolateral rotatory instability.
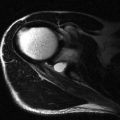
The ultrasound anatomy and examination techniques have been described previously. The characteristic findings in patients with CEO tendinopathy include loss of reflectivity and disorganization of the normal reticular fibre pattern within the involved tendons. The anterior part is affected more often than the posterior, and the deeper portions more than the most superficial. This pattern reflects the characteristic involvement of extensor carpi radialis brevis. As the disease progresses, ingrowth of abnormal vessels (neovascularization or angiogenesis) occurs and abnormal Doppler signal is commonly found ( Fig. 6.1 ). The degree of vascular ingrowth is so great in some patients, that it has been suggested that much of the high signal within the tendons identified on fat-suppressed T2-weighted MR images represents abnormal vessels. As tendon degeneration progresses, fibre disruption appears and areas of focal tendon delamination or partial tears are seen ( Fig. 6.2 ). The disease progresses to involve the adjacent tendons. Involvement of the radial collateral ligament may also occur and this is said to carry a poor prognosis for conservative management. With further progression, the tendon may begin to separate from its periosteal attachment ( Fig. 6.3 ) and ultimately rupture occurs. There appears to be a good correlation between active Doppler changes and areas of tendon delamination with patient symptoms ( Fig. 6.4 ).




Enthesopathy is the term used to describe pathological changes at the enthesis, the point where the tendon inserts into the lateral epicondyle. Occasionally this is distinct from tendinopathy but in practice the two coexist and often merge. Chronic enthesopathy is diagnosed when insertional bone changes are present at the tendon attachment. Such findings include calcification, which can assume several patterns: linear or conglomerates. With maturity the calcium deposits may ossify. Bony irregularity of the attachment site ( Fig. 6.5 ) leads to spur formation, visible on radiographs. It should be noted that bony changes at the enthesis may persist and become chronic and are, therefore, not necessarily associated with active symptoms. Active Doppler at the enthesis is a more helpful sign of an active problem.
| The ultrasound report of patients with CEO enthesopathy should confirm the diagnosis, indicate which tendons are involved and attempt to differentiate between simple tendinopathy and delamination/partial tears. Doppler activity and radial collateral ligament involvement help to stage the disease. |


Radial Collateral Ligament and Plica
The radial collateral ligament runs from the lateral epicondyle deep to the CEO proximally, to the lateral aspect of the neck of the radius distally, where it inserts on the annular ligament ( Fig. 6.7 ). Apart from being simultaneously involved in patients with CEO tendinopathy and traumatic injury, there are relatively few disorders that affect the ligament in isolation and it is relatively uncommon that imaging is required. The radial collateral ligament is not as easy to identify as the ulnar collateral ligament but it can be found on the deep aspect of the common CEO.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


