Olecranon Bursitis
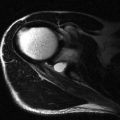
One of the commonest causes of localized pain in the posterior elbow is olecranon bursitis. This is usually a clinical diagnosis as bursa enlargement is easily palpable in the typical location above the olecranon. Occasionally in patients with large limbs, subtle enlargement may be difficult to detect clinically and imaging may be helpful in these cases ( Fig. 9.1 ).

The cause is usually due to repetitive friction as the characteristic location of the olecranon bursa makes it particularly susceptible to trauma, leading to haemorrhage within the bursa. Conditions associated with inflammatory synovitis also commonly affect the bursa ( Fig. 9.2 ). Septic bursitis, particularly related to penetrating injuries, also occurs.

The ultrasound findings are the same as bursitis elsewhere. The bursa may be well or poorly defined depending on the degree of inflammatory changes in the surrounding fat.
The contents of the olecranon bursa may be clear, anechoic, fluid in the case of a pure adventitial bursitis, or complex if haemorrhage or infection is present.
Occasionally aspiration and cortisone injection are carried out for simple or inflammatory bursitis, although the latter is controversial and may be associated with secondary infection and subcutaneous fat atrophy.
Triceps Tendinopathy and Rupture
Triceps tendinopathy is distinctly less common than biceps tendinopathy ( Fig. 9.3 ). Loss of structure, areas of delamination and increased Doppler are characteristic ( Fig. 9.4 ). Overuse syndromes are the most common. Ultrasound is particularly useful in detecting triceps tendinopathy due to impingement against orthopaedic hardware, where MRI is often unsuccessful. Tendon rupture is also rare and usually indicates an underlying condition predisposing to tendon degeneration, similar to those that might underlie biceps rupture. These include diabetes, systemic arthritis, renal failure or drug usage, particularly anabolic steroid use. Triceps rupture may also occur in association with olecranon bursitis, infection or following local steroid injections. As the separate insertion of the medial head is usually spared, tears are technically most commonly partial and involve the combined lateral and central heads.