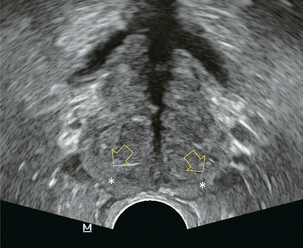
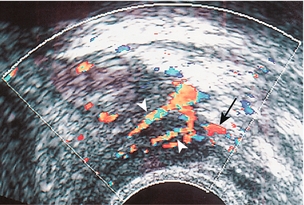
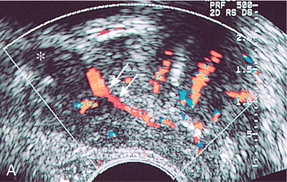
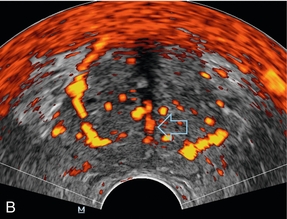
Chapter 11 The most important use of colour Doppler imaging of the prostate remains as an aid in cancer detection. This is particularly relevant in patients in whom cancer is suspected based on prostate specific antigen (PSA) elevation without obvious tumour on grey scale imaging. Other uses for Doppler imaging are largely confined to detection of prostatitis and inflammatory conditions. Controversy continues surrounding diagnosis and treatment of prostate cancer. This is largely attributable to the wide range of biological behaviour found with this disease. Up to 30% of 80-year-old males will have histological evidence of prostate cancer, yet most will die from other causes. Unfortunately, a more aggressive subset remains an important cause of mortality among men, with 33,720 deaths expected in the USA in 2011.1 The prostate lies immediately anterior to the rectum and inferior to the bladder. Prostatic zonal anatomy has been extensively described by McNeal.2 In summary, the prostate is composed of three major zonal areas; the peripheral zone, the central zone and the transition zone (Fig. 11-1). FIGURE 11-1 Axial ultrasound of the prostate in a normal patient. Note peripheral zone (*) separated from the more centrally oriented, periurethral, transition zone by the surgical capsule (open arrows). The prostate is supplied from two arterial sources: the prostatic arteries and the inferior vesical arteries, both arising from the internal iliac system. The prostatic arteries enter the prostate from an anterolateral location on each side, and give off capsular branches as well as urethral branches. Capsular arteries course along the lateral margin of the prostate, and give off numerous perforating branches which penetrate the capsule and supply approximately two-thirds of the total glandular tissue. The areas of penetration into the capsule are commonly referred to as the neurovascular bundles (Fig. 11-2). FIGURE 11-2 Axial image of the left neurovascular bundle. Note left neurovascular bundle (arrow) with perforating branches penetrating into the prostate. The inferior vesical arteries run along the inferior surface of the bladder and also provide urethral branches. In addition to supplying the central portion of the prostate, the inferior vesical arteries also give off branches which supply the bladder base, seminal vesicles and distal ureters (Fig. 11-3).3,4 FIGURE 11-3 (A) Sagittal image of the prostate at the level of the seminal vesicle (*) demonstrates periurethral flow (arrows) originating from the inferior vesicle artery. (B) Axial power Doppler image at the level of the mid prostate demonstrates branches of the inferior vesical artery (open arrow) supplying urethra and surgical capsule. Both the capsular and urethral branches can be visualised with colour Doppler ultrasound. In the absence of inflammation, neoplasm or hypertrophy, the normal prostate is expected to have low-level periurethral and pericapsular flow, with only a low level of flow in the prostatic parenchyma.5
Doppler Imaging of the Prostate
Indications
Anatomy
PROSTATE VASCULAR ANATOMY
Radiology Key
Fastest Radiology Insight Engine








