Chapter 7
Haemodialysis Access
Arteriovenous Fistulas and Synthetic Arteriovenous Grafts
At the end of 2009, there were 571,414 patients being treated for end-stage renal disease in the United States with 116,395 new cases in that year1; approximately 65% of these patients received haemodialysis.1 Complications associated with vascular access procedures are a major cause of morbidity and increasing healthcare costs in patients undergoing haemodialysis.2 For patients with end-stage real disease (ESRD) requiring haemodialysis, there are two options for vascular access, either the surgical creation of an arteriovenous fistula (AVF) or implantation of a synthetic arteriovenous graft (graft). Due to the lower rates of infection and thrombosis, mature AVFs are the preferred access when possible.3,4 Preoperative ultrasound evaluation of the upper extremity arteries and veins has been shown by several studies to increase the success rate of AVF creation by influencing surgical planning.5–7 While sonographic postoperative haemodialysis access evaluation may be beneficial in assessing AVF maturation,8,9 the role of postoperative ultrasound monitoring for early detection of access pathology allowing prompt intervention to increase the longevity of an access is still evolving.10–15
When clinically feasible and anatomically possible, the surgical creation of an AVF is preferred over a graft. Access placement in the non-dominant arm allows activities of daily living to continue as the non-dominant arm recovers; however, it is preferential to place a dominant arm AVF as opposed to a non-dominant arm graft in most patients. Potential haemodialysis access sites in decreasing order of preference are as follows: (1) forearm AVF (radiocephalic AVF or transposed forearm basilic vein to radial artery AVF); (2) upper arm brachiocephalic AVF or transposed brachiobasilic AVF; (3) forearm loop graft; (4) upper arm straight graft (brachial artery to upper basilic/axillary vein); (5) upper arm axillary artery to axillary vein loop graft; and (6) thigh graft. Other less common access configurations may also be utilised based on surgical experience.16 Cephalic vein use is preferred over a basilic vein transposition for fistula formation because the cephalic vein procedure involves less dissection and venous handling.
Preoperative Evaluation
Ultrasound exam optimisation has been previously reported.9,17–19 For evaluation of upper extremity arteries and veins, the patient should preferably be sitting upright. Following arterial assessment, a tourniquet is placed for evaluation of the veins20 (Fig. 7-1). The tourniquet should be repositioned on the arm above each level of examination, so those veins are maximally distended. Assessment of the internal jugular and subclavian veins should be performed with the patient supine for improved distension.

FIGURE 7-1 Photograph shows optimal patient positioning for preoperative upper extremity sonographic evaluation and tourniquet placement for evaluation of forearm veins. Sonographer is using a high-frequency 17 MHz transducer for best vascular visualisation.
The vascular structures are generally superficial and a high-frequency linear array transducer, at 12–15 MHz or higher, can provide good spatial resolution with adequate penetration. A light touch and plenty of coupling gel are recommended, so as to not deform the circular shape of the vessels. Preoperative criteria suggested by the literature include a minimum intraluminal arterial diameter of 2.0 mm (Fig. 7-2) and a minimal intraluminal venous diameter of 2.5 mm (Fig. 7-3) to allow successful AVF creation.5,9 Suggested criteria for graft creation include a minimum intraluminal venous diameter of 4.0 mm and a minimum arterial diameter threshold of 2.0 mm.5 In addition to diameter measurements, the caudal third of the brachial and radial arteries are evaluated for intimal thickening, calcification, stenosis or occlusion. Severity of arterial calcification may be categorised, depending on surgeon preference (Fig. 7-4). Evaluation for a normal triphasic or biphasic arterial waveform is performed, and peak systolic velocity (PSV) is measured in the region of artery planned for use (Fig. 7-5). If two arteries with paired veins are seen in the upper arm, a high radial artery take-off from the brachial artery should be suspected (Fig. 7-6). These arteries should be followed into the forearm to confirm high radial artery take-off and to exclude a prominent arterial branch supplying the elbow.
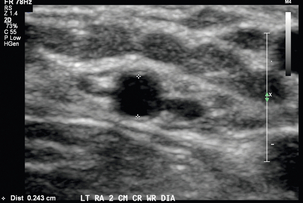
FIGURE 7-2 Greyscale transverse image of the left radial artery at the wrist demonstrates with caliper placement an intraluminal diameter of 2.4 mm satisfactory for access placement. Note use of high-frequency transducer and optimised technique.
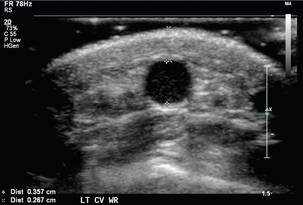
FIGURE 7-3 Greyscale transverse image of the forearm cephalic vein at the wrist demonstrates with (+) caliper placement an intraluminal diameter of 3.6 mm and with (×) caliper placement a distance of 2.7 mm from skin surface to anterior venous wall.
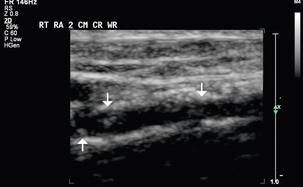
FIGURE 7-4 Greyscale longitudinal image shows calcifications in the caudal third of this right radial artery (arrows).
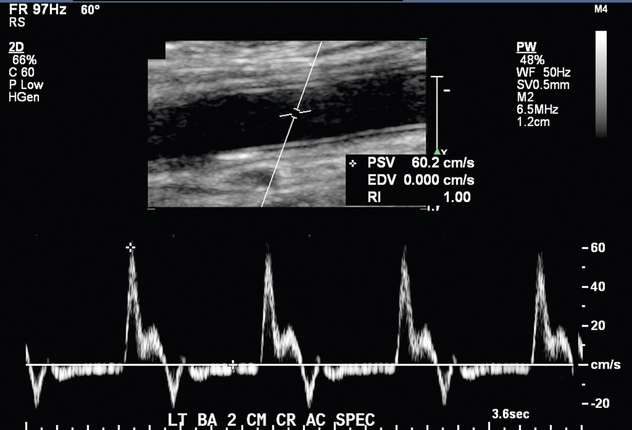
FIGURE 7-5 Spectral Doppler image shows a normal biphasic arterial waveform of this left brachial artery just above the antecubital fossa. PSV 60.2 cm/s.
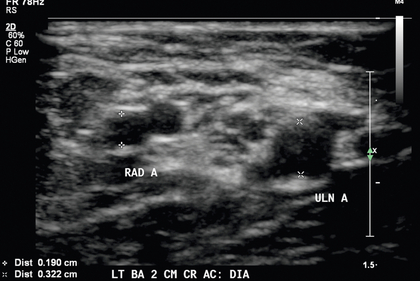
FIGURE 7-6 High bifurcation of the brachial artery should be suspected when two arteries are present near the antecubital fossa. Calipers (+) denote the radial artery (RAD A) and calipers (×) denote the ulnar artery (ULN A).
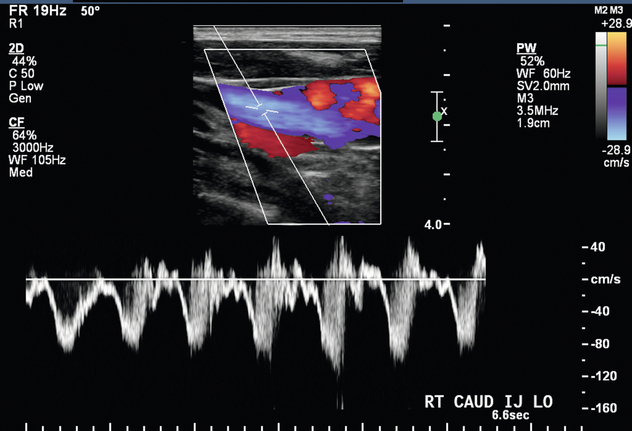
Venous assessment is performed with a tourniquet in place, and each vein should be visually inspected and compressed along the entire venous length to exclude thrombus. Internal transverse diameters of the cephalic vein are measured in the forearm at multiple levels. Internal diameters of the cephalic and basilic veins are measured in the upper arm at multiple levels in a similar fashion. The axillary vein, subclavian vein, and internal jugular vein should be assessed for compressibility and/or normal waveforms (Fig. 7-7).
Postoperative Ultrasound Evaluation
A surgically created dialysis access can have a variety of complications, and most of these can be identified and evaluated by ultrasound. Prior to the sonographic evaluation of a haemodialysis access, pertinent patient history and surgical notes are reviewed. An initial cursory ultrasound scan is performed to obtain an overview of the haemodialysis access. Once the general layout is understood, sonographic assessment is performed with greyscale and Doppler. The caudal third of the feeding artery is assessed for possible stenosis, and the intraluminal diameter is measured in the transverse plane. Colour and spectral Doppler assessment of the feeding artery is performed in the longitudinal plane to confirm the presence of normal low-resistance flow (Fig. 7-8). The anastomosis(es) are evaluated with both colour and spectral Doppler to assess for stenosis. The draining vein of the AVF or graft is inspected for wall thickening, stenosis, and thrombosis along its entire length. For a fistula, the intraluminal draining vein diameter and the vein depth from skin surface are measured at several points cranial to the arteriovenous anastomosis. A depth greater than 5 mm may suggest the need for superficialisation to improve accessibility. The draining vein is evaluated for accessory vein branches (Fig. 7-9





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


